(UroToday.com) The 2022 EAU Section of Oncological Urology (ESOU) Annual Meeting included a session on the early detection and personalized management of testis cancer and a presentation by Dr. Robert Huddart discussing follow-up of early stage seminoma. Dr. Huddart notes that there are several reasons why we follow-up patients after treatment of testicular cancer, including detection of recurrence, patient assurance, detection and management of late side effects, and for research purposes. However, we must hit the sweet spot and find the balance between detection of relapse and the cost, resource use, radiation exposure, and scan anxiety associated with follow-up. According to standard UK seminoma surveillance protocol, there is a risk of 1 in 300 for a second malignancy related to imaging alone.
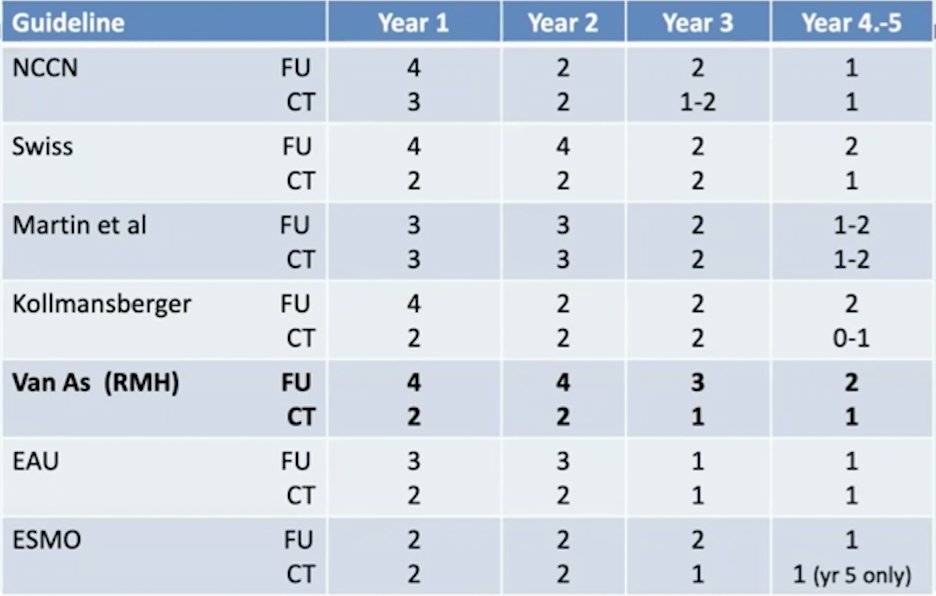
To attempt to potentially change intensity of follow-up, it is important to understand patterns of recurrence. In an assessment of 2,466 patients with stage I seminoma enrolled in randomized trials, 7/11 of carboplatin relapses were at ~24 months detected by scheduled abdominal CT and 4 relapses (0.2% of all patients randomized) occurred at > 3 years follow-up.1 Furthermore, there is significant heterogeneity in seminoma surveillance protocols, as highlighted in the following figure:
Dr. Huddart and his group recently presented (GU ASCO 2021) results of the Trial of Imaging and Surveillance in Seminoma Testis (TRISST, NCT00589537), which was designed to assess whether CTs can safely be reduced, or replaced with MRI, without an unacceptable increase in advanced relapses. TRISST is a phase III, multicenter, non-inferiority, factorial trial. Eligible men had undergone orchiectomy for stage I seminoma with no adjuvant therapy planned. Randomization was to:
- 7 CTs: 6, 12, 18, 24, 36, 48, 60 months after randomization
- 7 MRIs: 6, 12, 18, 24, 36, 48, 60 months after randomization
- 3 CTs: 6, 18, 36 months after randomization
- 3 MRIs: 6, 18, 36 months after randomization

Follow-up for the trial was for 6 years with a primary outcome of 6-year incidence of stage ≥IIC relapse, aiming to exclude an increase ≥5.7% (from 5.7% to 11.4%) with MRI (versus CT) or 3 scans (versus 7). The target sample size was 660 patients, all contributing to both comparisons. Secondary outcomes include relapse ≥3cm, disease-free and overall survival.
There were 669 men enrolled from 35 UK centers (2008-2014), with a mean tumor size of 2.9 cm, and 358 (54%) were low risk (≤4cm, no rete testis invasion). In those patients remaining on surveillance, compliance was good with 94% of scans attended, 79% on time (+/- 4 weeks). Median follow-up was 72 months over which 82 (12%) patients relapsed. Incidence of stage ≥IIC relapse was low in all groups (n=10). More events occurred with 3 scans compared to 7 scans, though non-inferior based on design criteria: 9 (2.8%) versus 1 (0.3%), 2.5% increase (90% CI 1.0% to 4.1%; intent-to-treat). In the 3-scan arms 4/9 relapses could potentially have been detected earlier with the 7-scan schedule:

Fewer events occurred with MRI versus CT: 2 (0.6%) versus 8 (2.5%), 1.9% decrease (90% CI -3.5% to -0.3%; intent-to-treat). Incidence of relapse ≥3cm was 3.7% and non-inferiority was shown for both comparisons:

In all groups, most relapses were detected at scheduled imaging, very few occurred beyond 3 years (5 in 558 at risk, <1%):

Relapse treatment outcomes were good (81% complete response) with no tumor-related deaths. Treatment for stage >=IIC was typically BEP x3 or BEP x4, although 16/72 (22%) of patients with lower stage also received BEP. 5-year disease free survival was 87% and for overall survival 99% and similar across groups. Dr. Huddart’s conclusions from TRISST were that (i) incidence of advanced relapse was very low regardless of imaging modality or frequency, (ii) treatment for relapse was successful and long-term outcomes were excellent in all arms, with no deaths due to testicular cancer, (iii) MRI is non-inferior to CT, avoids irradiation and should be recommended, (iv) a 3-scan schedule was non-inferior to 7 scans, and (v) relapses beyond 3 years was rare.
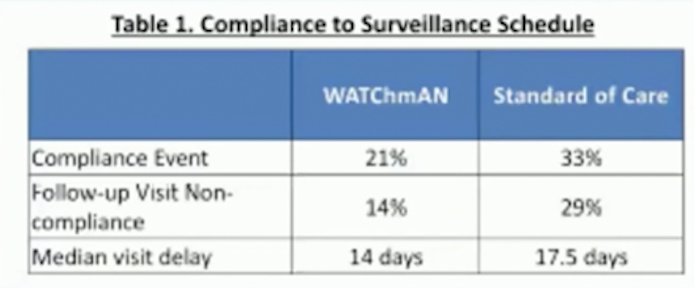
One of the worries when placing these young men on surveillance protocols is the concern regarding follow-up compliance. There are several reasons why men may not comply with follow-up, including feeling well, work/life factors, mobility, avoidance, and cost (particularly if care is not publically funded). With the COVID-19 pandemic, there has been a general push for increasing utilization of telehealth, which may be advantageous for testicular cancer patients. Dr. Huddart notes that since 2014, the Royal Marsden Hospital offers ‘virtual’ follow-up for patients who are >2 years from their diagnosis. These patients have tumor markers and imaging done and then a phone call to check results, with a complete checklist to include ensuring self-examination. In situations where imaging or blood work may be concerning, the patient is then seen as a normal clinic visit at the next follow-up. Work out of the Princess Margaret Cancer Centre, presented at GU ASCO 2020, assessed a randomized trial of virtual surveillance versus standard of care for clinical stage I testicular cancer (WATChmAN trial), whereby stage I germ cell tumor patients were randomized to standard of care clinical follow- versus a web-based online asynchronous follow-up clinic. Patients in the web-based online asynchronous follow-up clinic only had a 14% rate of non-compliance compared to 29% in the standard follow-up clinic:
Dr. Huddart concluded his presentation with the following take-home messages:
- There are limited studies that have looked at the optimal follow-up schedule for testicular seminoma
- There is a wide variation of recommended schedules
- There must be a balance between detecting recurrence, radiation exposure, and resource use
- Late effect care is a neglected area
- Research is needed on new models of care
Presented by: Professor Robert A. Huddart, Institute of Cancer Research and Royal Marsden Hospital, Sutton, Surrey, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 EAU Section of Oncological Urology (ESOU) Hybrid Annual Meeting, Madrid, Spain, Fri, Jan 21 – Sun, Jan 23, 2022.
References:
- Mead GM, Fossa SD, Oliver RTD, et al. Randomized Trials in 2466 Patients with Stage I Seminoma: Patterns of Relapse and Follow-up. J Natl Cancer Inst. 2011 Feb 2;103(3):241-249.