MRI of renal cysts gives us better resolution, contrast, and better characterization in general, using the Bosniak classification. MRI will allow us to characterize and differentiate between benign renal masses (AML, oncocytoma and others) and malignant tumors (clear cell, papillary, and chromophobe renal cell carcinoma [RCC]).
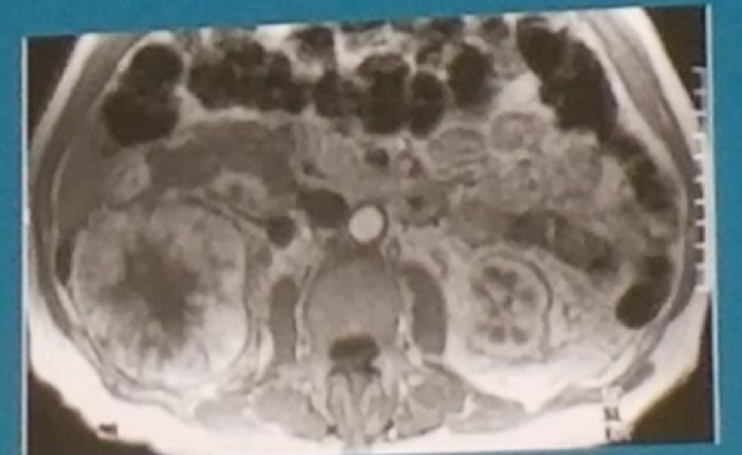
MRI of an AML will demonstrate macroscopic fat (figure 1), a hypersignal on T1 images and hyperintense signal if fat rich AMLs in T2. The DCE phase of MRI will show early, intense enhancement. When the AML is lipid poor, it is difficult to distinguish it from RCC.
Oncocytoma in MRI will manifest as a homogenous mass if it is smaller than 3 cm, but when larger than 3 cm, it will often display a central scar with spoke wheel appearance (Figure 2). It is commonly a peripheral lesion, with well defined limits and with similar characteristics as RCC. T1 will demonstrate low signal intensity, while T2 will show high signal intensity. The DCE phase will demonstrate the highest washout rate.
Clear cell RCC in MRI has a low signal on T1, and heterogenic signal on T2 due to necrosis, cystic degeneration, and/or hemorrhage. The could be a small amount of intracellular fat. DCE will display hypervascular heterogenous lesion, with possible central necrosis. Papillary RCC in MRI is usually a well circumscribed homogenous peripheral lesion, with a fibrous capsule with low intensity signal on T1 and T2. DCE will show a hypovascular lesion with progressive enhancement. Lastly, Chromophobe RCC has no clear features, but with a tendency to be well circumscribed and homogenous. T2 shows variable signal intensity, and DCE will demonstrate intermediate enhancement with a central stellate scar.
Multiparametric MRI might be useful in assessing renal masses, using the T1/T2 weighted imaging, dynamic contrast enhanced imaging, diffusion weighted imaging (DWI) and others. DWI is a promising modality for renal masses, but is still not ready for routine clinical use. This is due to its limitations, including differences in ADC value thresholds, lack of standardization of the MRI and lack of experience.
Eventually, even when perfected, imaging is not enough and histologic confirmation is still needed. The future will entail development of radiomics which will enable correlation of function to imaging.
Figure 1: MRI of AML
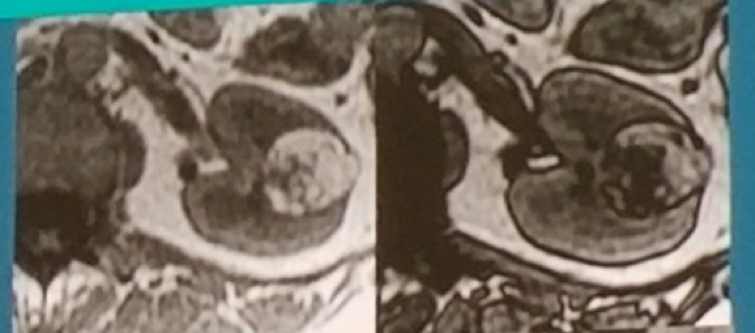
Figure 2: MRI of Oncocytoma:
Speaker: Jochen Walz, MD Assistant Professor Paoli-Calmettes Institute Cancer Centre, Urology, Marseilles, France
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at The 15th Meeting of the EAU Section of Oncological Urology ESOU18 - January 26-28, 2018 - Amsterdam, The Netherlands