(Urotoday.com) The newly formed Global Society of Rare Genitourinary Tumors (GSRGT) held its inaugural meeting, focusing on penile and testicular cancer. The session held Saturday, December 12th focused on testis cancer. In this session, Dr. Robert Hamilton presented on the management of early-stage (CSI) seminoma, focussing on existing guidelines including the role of surveillance, prognostic factors, radiotherapy, carboplatin and future directions.
Dr. Hamilton highlighted guidelines from the Canadian Urological Association (CUA), American Urological Association (AUA), National Comprehensive Cancer Network (NCCN), and European Association of Urology (EAU). Notably, all North American guidelines have endorsed non-risk adapted surveillance for patients with clinical stage I seminoma, while the EAU guidelines appear to only emphasize this approach in patients with no risk factors.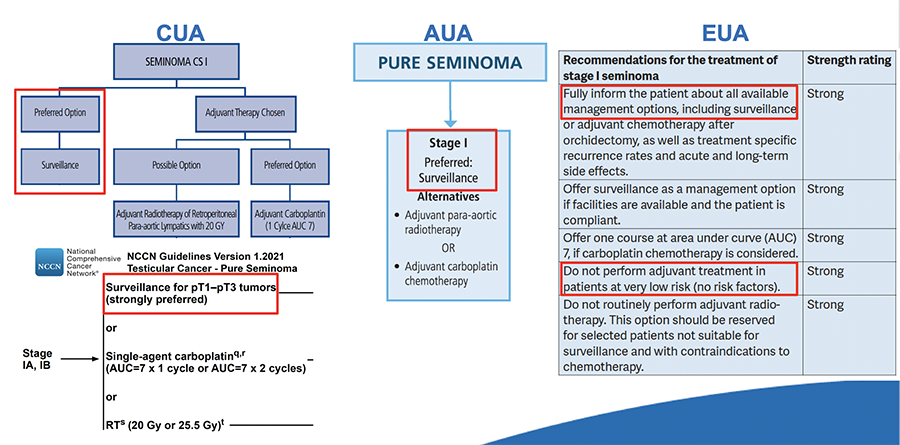
He then highlighted data supporting surveillance in this population, given that only 15% of patients treated with this approach relapse and the vast majority can be successfully salvaged. Even considering this need for salvage therapy, he emphasized that the total treatment burden is lower with an initial surveillance approach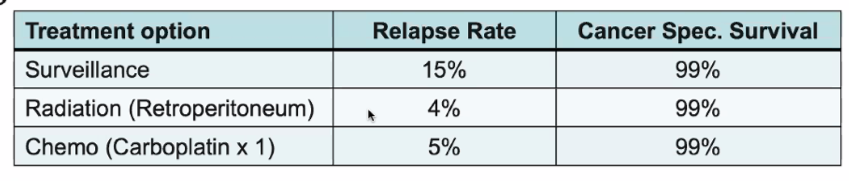
While the initial approach to surveillance utilized a risk-adapted approach, subsequent data demonstrated no association between rete testis invasion and the risk of relapse while tumor size was continuously associated with the risk of relapse, without clear cut-offs.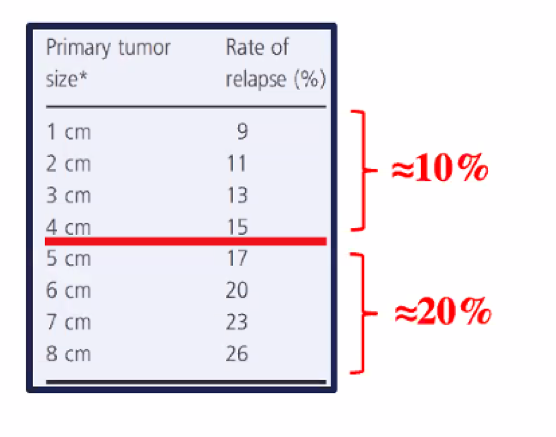
As a result, subsequent systematic reviews cautioned that size and rete testis invasion have significant limitations in their prognostic value and caution is warranted for their clinical use.
An alternative to surveillance is radiotherapy. Dr. Hamilton highlighted that, while radiotherapy reduces the risk of relapse from approximately 15% to 5%, it is associated with a significant risk of secondary cancers and cardiovascular disease. Further, ongoing surveillance of the retroperitoneum is required for relapse. Thus, in both Ontario data and American data from the NCDB, utilization of adjuvant radiotherapy has been declining over time.
The third treatment option is chemotherapy. The MRC TE19 trial compared para-aortic radiotherapy to one cycle of carboplatin and concluded that carboplatin was non-inferior. However, Dr. Hamilton highlighted five different concerns with this approach with a particular focus on the relatively modest reductions in relapse risk reduction and the potential for adverse biology following adjuvant carboplatin.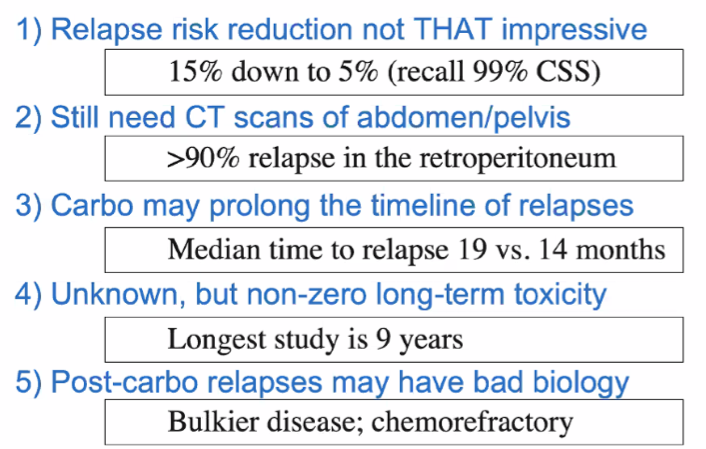
Focussing first on the relapse risk reduction, he highlighted data from SWENOTECA demonstrating relatively modest risk reductions with the use of carboplatin, compared to surveillance.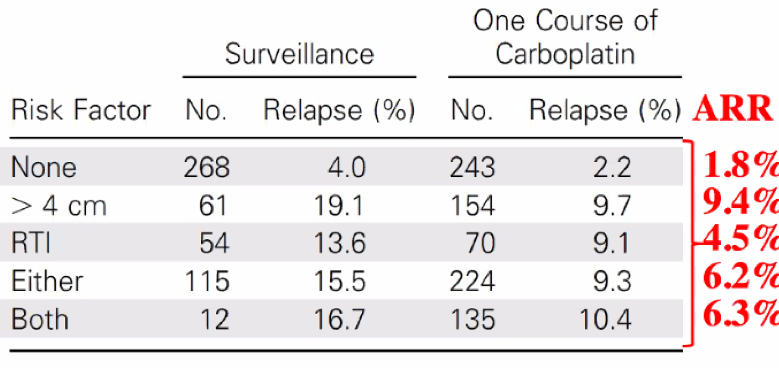
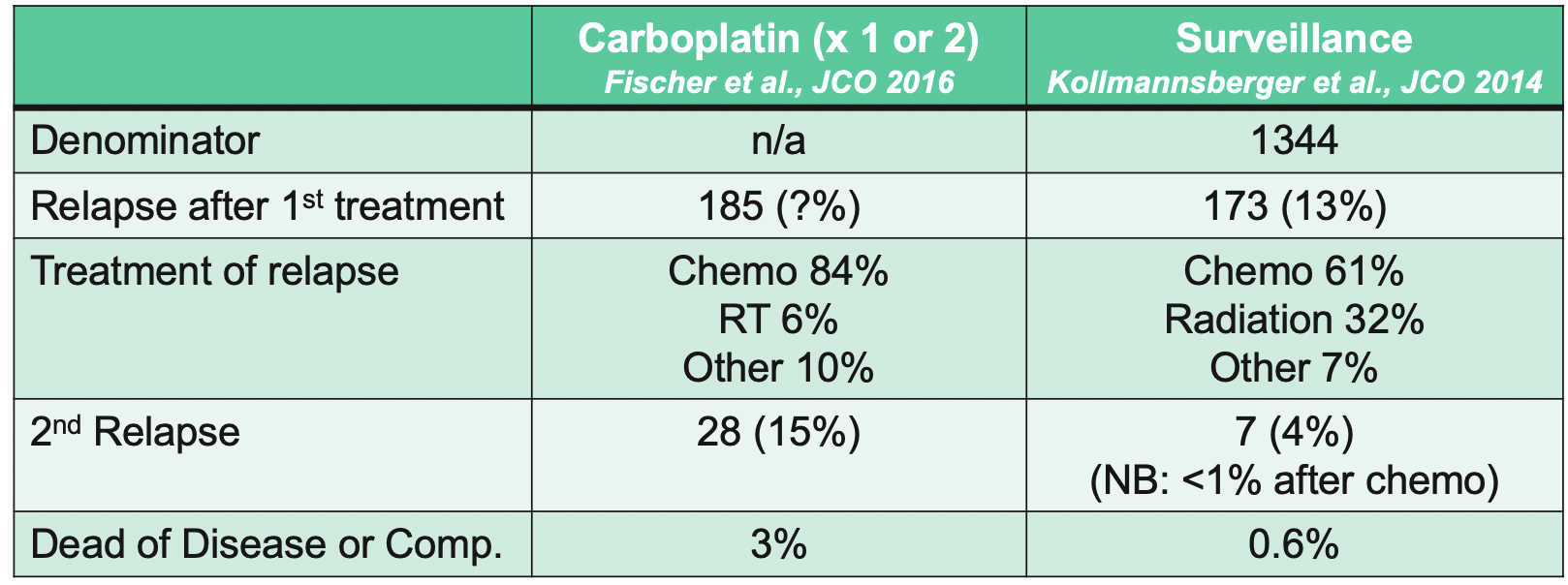
He then discussed the potential for adjuvant carboplatin to induce chemorefractory disease. While there are no direct data to inform this, a qualitative comparison of patients who had relapse following adjuvant carboplatin to those with relapse following surveillance suggests that second relapses may be more common and associated with higher rates of death from disease or complications.
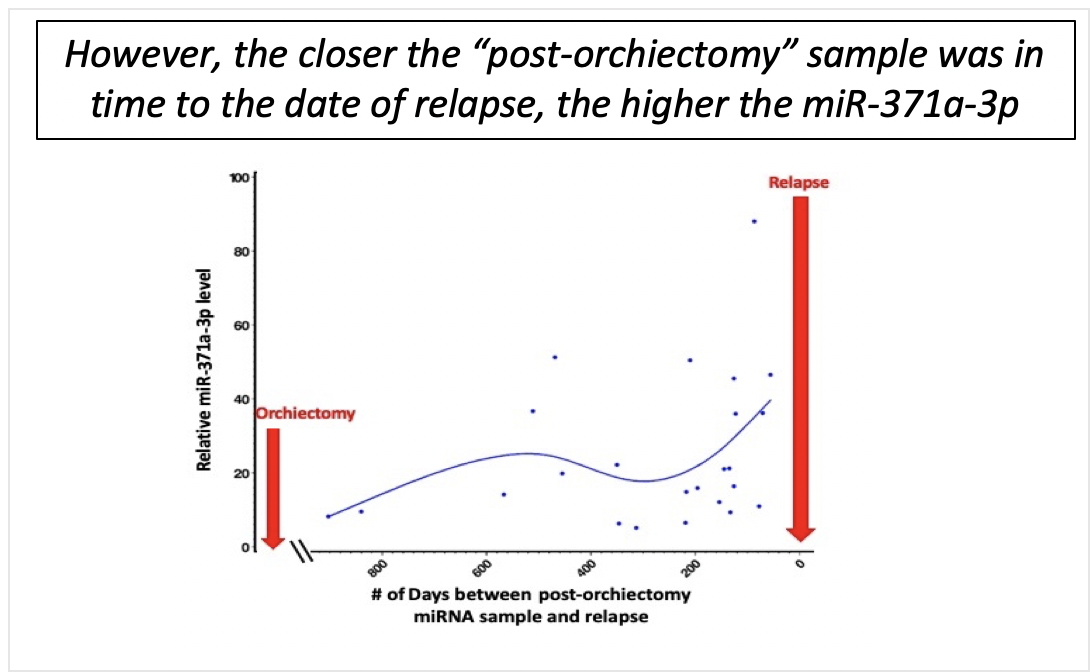
Looking to the future, Dr. Hamilton discussed the potential for data on the role of retroperitoneal lymph node dissection (RPLND) in stage II seminoma to change the paradigm of surveillance with the use of RPLND for salvage of surveillance failures while sparing the systemic toxicity of chemotherapy and radiotherapy. Further, he highlighted the potential role of miRNA-371. In this clinical setting, it would be ideal to show that initial post-orchiectomy miR levels can risk stratifying patients’ likelihood of relapse. However, he showed early data from his own group showing that initial post-operative miR371 levels were not able to discriminate patients who were destined to relapse from those who were not. However, rises in miR371 presaged clinical relapse.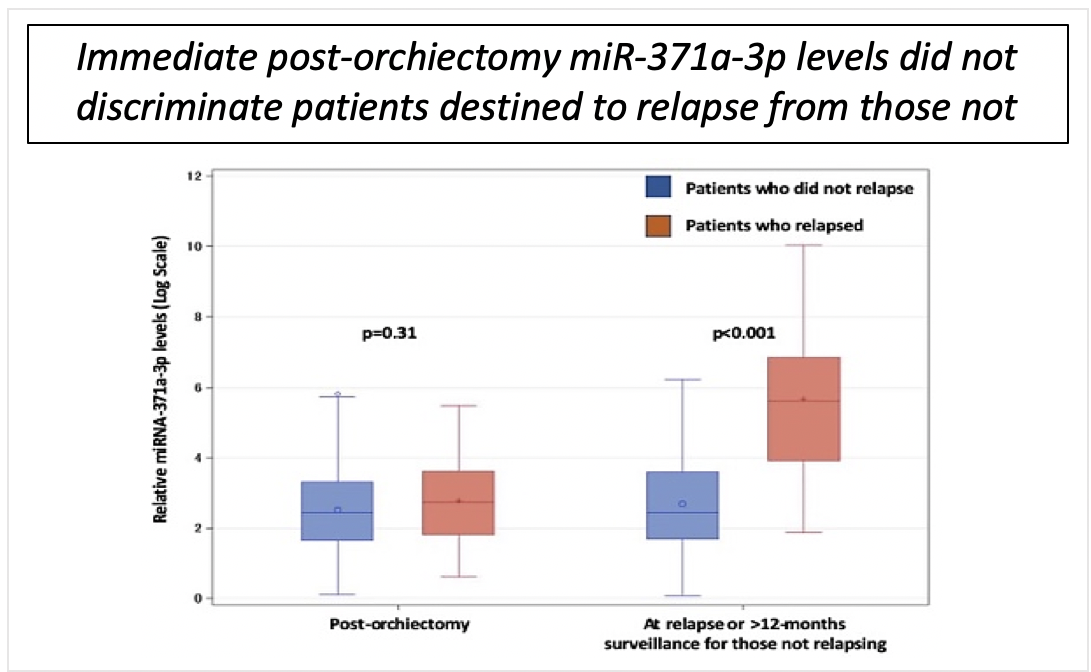
In conclusion, Dr. Hamilton highlighted that outcomes for patients with clinical stage I seminoma are excellent without good prognostic factors to distinguish a high-risk group. Given concerns with the toxicity of radiotherapy and chemotherapy, surveillance should be preferred for most. Finally, the future of CSI seminoma is likely to evolve with a greater role for surveillance if RPLND is effective for relapse.
Presented by: Robert J. Hamilton, MD MPH FRCSC, Associate Professor, University of Toronto, Princess Margaret Cancer Centre
Written by: Christopher J.D. Wallis, MD, Ph.D., Instructor in Urology, Vanderbilt University Medical Center, Nashville, Tennessee @WallisCJD on Twitter during the 1st Global Society of Rare Genitourinary Tumors Virtual Summit, December 11-12, 2020