(UroToday.com) The 2024 IBCN annual meeting included a session on novel therapies and outcome measures in clinical trials, featuring a presentation by Dr. Gautier Marcq discussing the benefit of whole-pelvis radiation for patients with muscle-invasive bladder cancer. The value of pelvic lymph node irradiation is debated for patients with muscle-invasive bladder cancer undergoing curative-intent radiation therapy.
Moreover, it is noted that surgical cohorts have a rate of lymph node invasion of 20%-30%. Radiotherapy is often offered to patients with higher-risk muscle-invasive bladder cancer, usually associated with: higher cT, hydronephrosis, cN+, CIS, LVI, and pelvic lymph node invasion. Dr. Marcq and colleagues sought to compare the oncological outcomes between bladder-only radiation therapy versus whole-pelvis radiation therapy using a large Canadian multicenter collaborative database.
The study cohort consisted of 809 patients with muscle-invasive bladder cancer (cT2-4aN0-2M0) who underwent curative radiation therapy at academic centers across Canada. Patients were divided into two groups based on the radiation therapy volume: whole-pelvis radiation therapy versus bladder-only radiation therapy. The median follow-up in this cohort was 54 months (95% CI 46-60). Inverse probability of treatment weighting (IPTW) and absolute standardized differences were used to balance covariates across treatment groups. Regression models were used to assess the impact of the radiation therapy volume on the rates of complete response, cancer-specific survival, and overall survival:
After exclusion criteria, 599 patients were included, of whom 369 (61.6%) underwent whole-pelvis radiation therapy. Patients receiving whole-pelvis radiation therapy were younger (absolute standardized difference 0.41) and more likely to have an ECOG performance status of 0-1 (absolute standardized difference 0.21), clinical node-positive disease (absolute standardized difference 0.40), and lymphovascular invasion (absolute standardized difference 0.25). In addition, whole-pelvis radiation therapy patients were more commonly treated with neoadjuvant chemotherapy (absolute standardized difference 0.29) and concurrent chemotherapy (absolute standardized difference 0.44). In the IPTW cohort, bladder-only radiation therapy and whole-pelvis radiation therapy groups were well balanced (all pre-treatment parameters with an absolute standardized difference < 0.10):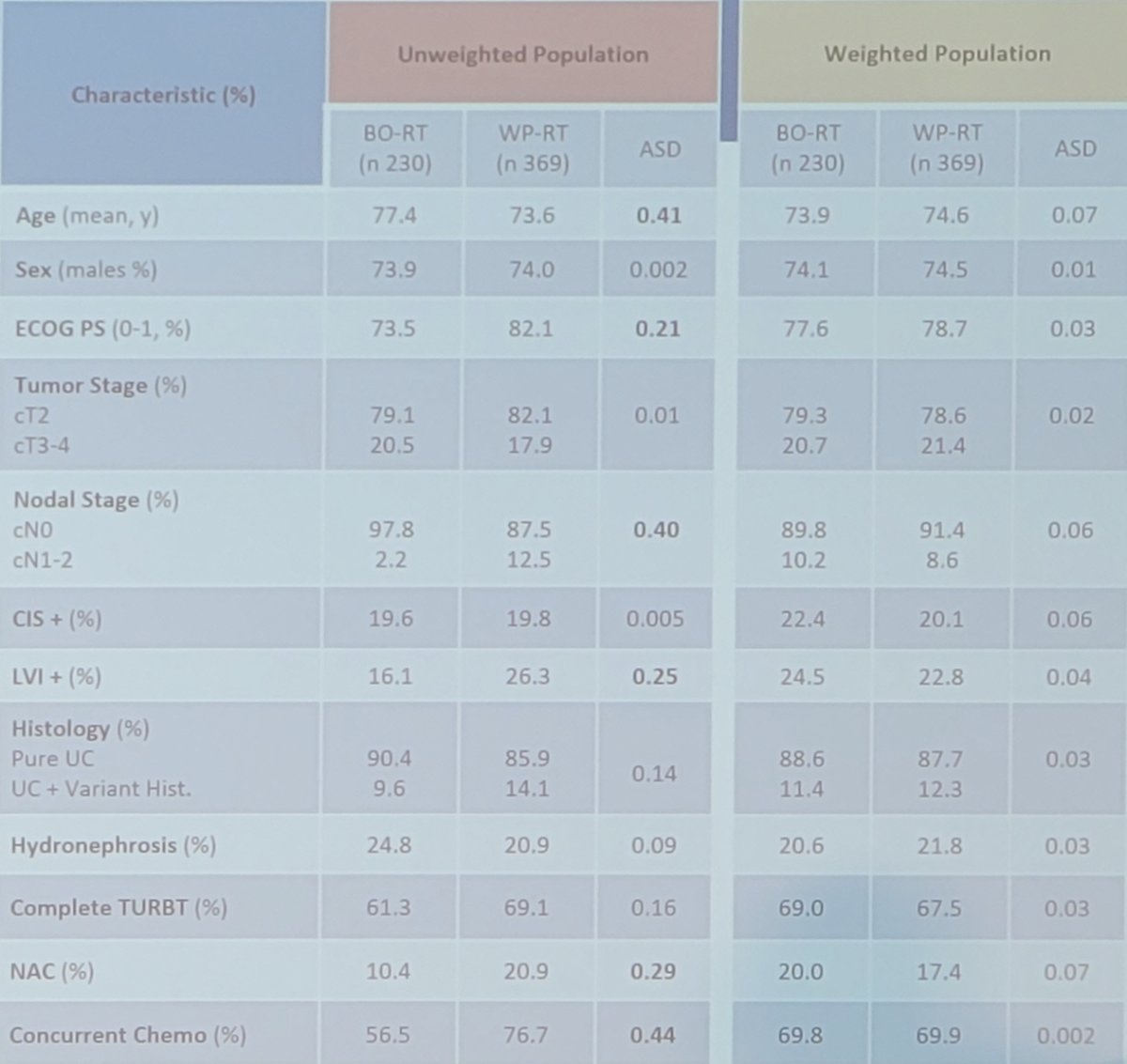
Approximately 3 months post radiotherapy, 407 patients (76%) had achieve a complete response. In multivariable analysis, hydronephrosis (OR 0.45, 95% CI 0.28-0.71) was the sole predictor of a lower odds of complete response. Whole-pelvis radiation therapy was not associated with complete response rates post-radiation therapy (OR 1.14, 95% CI 0.76-1.72; p = 0.526) but was associated with both cancer-specific survival (HR 0.66, 95% CI 0.47-0.93; p = 0.016) and overall survival (HR 0.68, 95% CI 0.54-0.87; p = 0.002), independent of other prognostic factors:
Dr. Marcq and colleagues also performed several sensitivity analyses (T2-T3 cN0 cM0, TMT, hypofractionated regimen) and the results were consistent, demonstrating an improved survival for whole-pelvis radiation therapy.
Dr. Marcq concluded his presentation discussing the benefit of whole-pelvis radiation for patients with muscle-invasive bladder cancer with the following take-home points:
- Pelvic lymph node involvement may improve survival
- Prospective validation is required, although unlikely to happen
- The study is limited by the retrospective design and multiple radiotherapy regimens
Presented by: Gautier Marcq, MD, MSc, McGill University Medical Centre, Montreal, Quebec, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, WellStar MCG Health, @zklaassen_md on Twitter during the 2024 International Bladder Cancer Network (IBCN) Annual Meeting, Bern, Switzerland, Thurs, Sept 19 – Sat, Sept 21, 2024