(UroToday.com) The 2024 PSMA conference featured a presentation by Dr. Matthew Rettig discussing the treatment landscape of mCRPC.
Dr. Rettig started his presentation by emphasizing that prostate cancer results in >34,000 deaths each year, with a man dying of prostate cancer in the US every 15 minutes. Of note, the mortality of breast cancer is ~42,500 deaths per year, but with 2.5 times the NCI funding compared to prostate cancer:
Dr. Rettig notes that the prostate cancer journey typically lasts 10-15 years, with mCRPC being the final disease state before mortality. In the United States, ~90% of patients present prior to mCRPC. From 1981 to 2023, we have a plethora of FDA approved agents for mCRPC, with the likely possibility that 177Lu-PSMA-617 is approved in 2024:

Each of these agents can be grouped into the following categories of therapy:
- Hormonal (androgen receptor pathway blockers):
- Abiraterone
- Enzalutamide
- Cytotoxic:
- Docetaxel
- Cabazitaxel
- Immunotherapeutic: Sipuleucel-T
- DNA damage: Radium-223
- Biomarker-directed:
- Pembrolizumab
- Olaparib
- Rucaparib
- 177LuPSMA-617
The following table summarizes the mCRPC overall survival benefit among the FDA approved treatments:
Dr. Rettig emphasized that we know that precision oncology leads to better outcomes. This may include:
- Metastatic biopsy: whole exome/transcriptome assessment, targeted analysis of actionable genomic lesions, and DNA methylation
- Plasma: targeted analysis of circulating tumor DNA (ie. AR, BRCA1/2, ATM)
- Circulating tumor cells: targeted analysis of circulating tumor cells (ie. AR-V7, expressional profiles, single cell sequencing)
- Imaging: functional evaluation (ie. NaF, DHT, PSMA)
The two trials that utilize imaging as a biomarker, include the VISION1 phase III trial and the TheraP2 phase II trial. Although both of these trials utilized 68Ga-PSMA-11, Dr. Rettig emphasized that the NCCN guidelines note that both 68Ga-PSMA-11 or 18F-piflufolastat PSMA imaging can be used to determine eligibility for 177Lu-PSMA-617 therapy based on multiple reports describing the equivalency of these imaging agents.
TheraP was the first randomized study to evaluate 177Lu-PSMA-617 vs cabazitaxel for men with mCRPC after docetaxel. In this open label, phase II trial, 200 men were randomized to either 177Lu-PSMA-617 or cabazitaxel. The primary endpoint of this study was a PSA decline of 50% (PSA50) and after a median follow up of 13 months, 177Lu-PSMA-617 significantly improved PSA-PFS compared with cabazitaxel (HR 0.63, 95% CI 0.46 to 0.86) and a had a much higher PSA50 rate (66% vs 37%):
The VISION trial evaluated 177Lu-PSMA-617 in men with PSMA-positive mCRPC who had previously received treatment with a next-generation androgen receptor signaling inhibition (abiraterone, enzalutamide, etc) and one or two prior lines of taxane chemotherapy. There were two alternate primary endpoints: rPFS and OS. Treatment with 177Lu-PSMA-617 + standard of care significantly improved OS by a median of 4.0 months (median OS: 15.3 vs 11.3 months; HR 0.62, 95% CI 0.52 to 0.74; p < 0.001, one-sided), compared to standard of care alone.
For rPFS, treatment with 177Lu-PSMA-617 + standard of care significantly improved rPFS by a median 5.3 months (median rPFS, 8.7 vs 3.4 months; HR 0.40, 99.2% CI 0.29 to 0.57; p < 0.001, one-sided):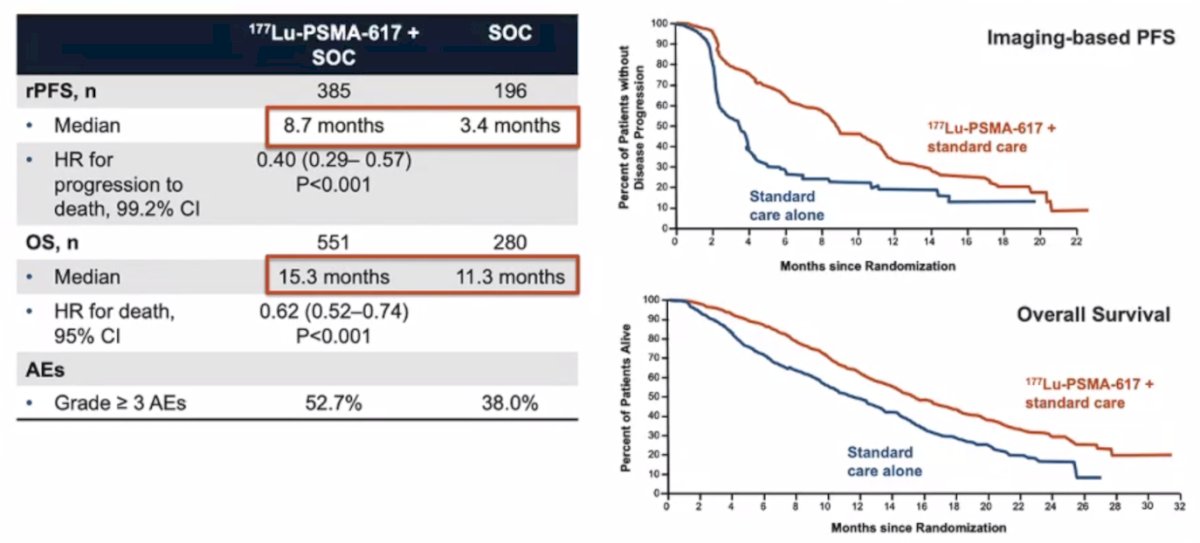
Dr. Rettig notes that it is important to understand the difference between germline and somatic mutations. Germline mutations occur at the parental gamete level and the entire organism carries the mutation, whereas somatic mutations occur downstream and affect only a small area of the organism: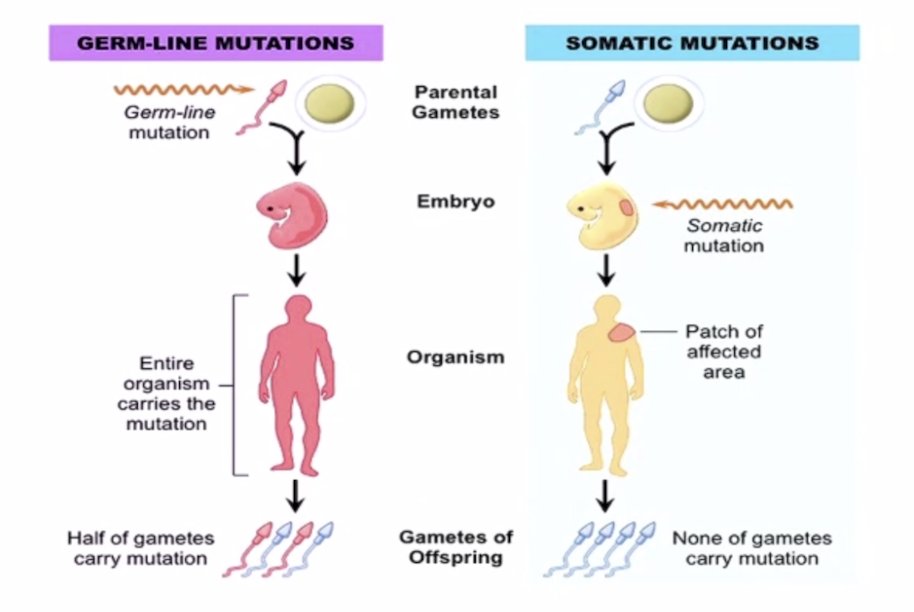
With regards to somatic mutation testing in prostate cancer, Dr. Rettig notes that we should be testing all men with mCRPC. Although current treatment selection for mCSPC is not based on sequencing results, it is important to consider sequencing for mCSPC to avoid unfruitful testing of aged specimens. For germline testing, we should be testing several groups of patients:
- >= High risk patients
- Intermediate risk with intraductal/cribriform histology (increased risk of homologous recombination deficiency)
- Earlier stages based on family history, ancestry, or personal history
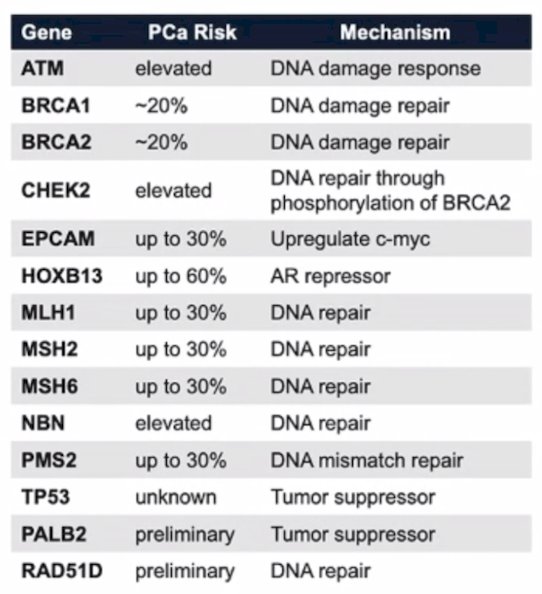
Data from Pritchard and colleagues suggest that BRCA2 mutant prostate cancer has more aggressive biology, men with germline mutations may not have any family history, and germline mutations occur in 11.8% of metastatic disease versus 4.6% of localized disease.3 Dr. Rettig notes that most hereditary prostate cancer genes encode proteins involved in DNA repair. However, the absence of a somatic mutation does not preclude the presence of a germline mutation. The following table highlights genes that cause hereditary prostate cancer:
Dr. Rettig then briefly discussed several of the precision oncology PARP inhibitor trials. First, TALAPRO-2 was a phase III RCT evaluating talazoparib and enzalutamide in the first line treatment setting for mCRPC patients.4 At a median follow-up of 16.8-17.5 months, the combination of talazoparib + enzalutamide was associated with significant improvements in rPFS with a median rPFS not reached in the intervention arm versus 13.8 months in the placebo/enzalutamide arm (HR: 0.45, 95% CI: 0.33 – 0.81, p<0.0001). In patients with HRR gene status of non-deficient or unknown, the HR was 0.70 (95% CI 0.54-0.89):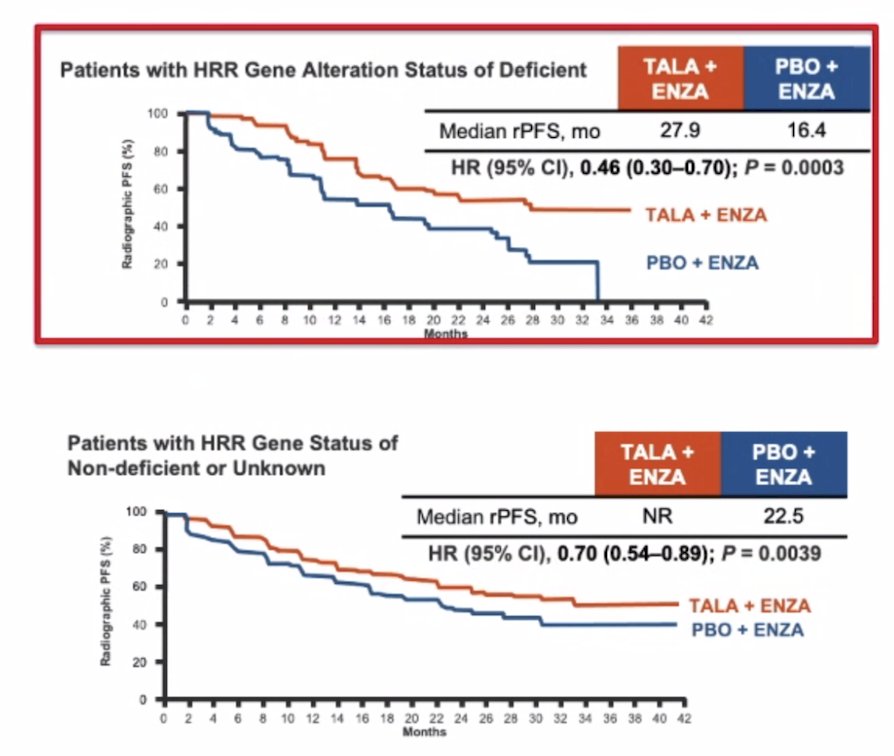
PROpel was a phase 3 trial of first-line olaparib + abiraterone acetate + prednisone versus placebo + abiraterone acetate + prednisone in mCRPC patients, with a primary endpoint of rPFS.5 This trial found a 34% risk reduction of progression of death with the olaparib + abiraterone acetate + prednisone arm (HR 0.66, 95% CI 0.54 – 0.81):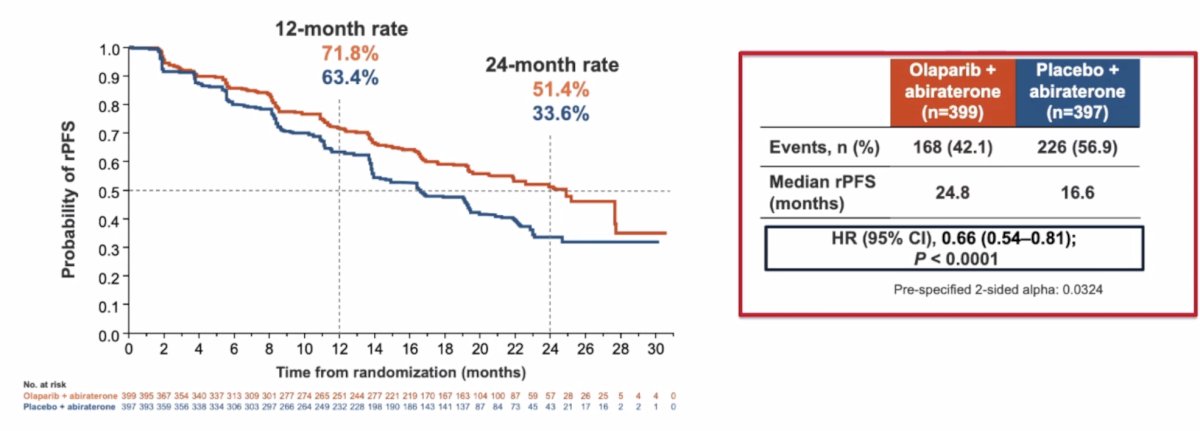
Finally, the phase 3 MAGNITUDE trial assessed first-line niraparib + abiraterone acetate + prednisone versus placebo + abiraterone acetate + prednisone for mCRPC +/- HRR gene alterations, with a primary endpoint of rPFS.6 This combination led to a 47% risk reduction of progression of death with niraparib + abiraterone acetate + prednisone (HR 0.53, 95% CI 0.36-0.79):

Another trial discussed by Dr. Rettig was the ACIS trial, which assessed apalutamide + abiraterone acetate + prednisone versus placebo + abiraterone acetate + prednisone in mCRPC.7 This trial found that the addition of apalutamide improved rPFS, but not overall survival among these patients: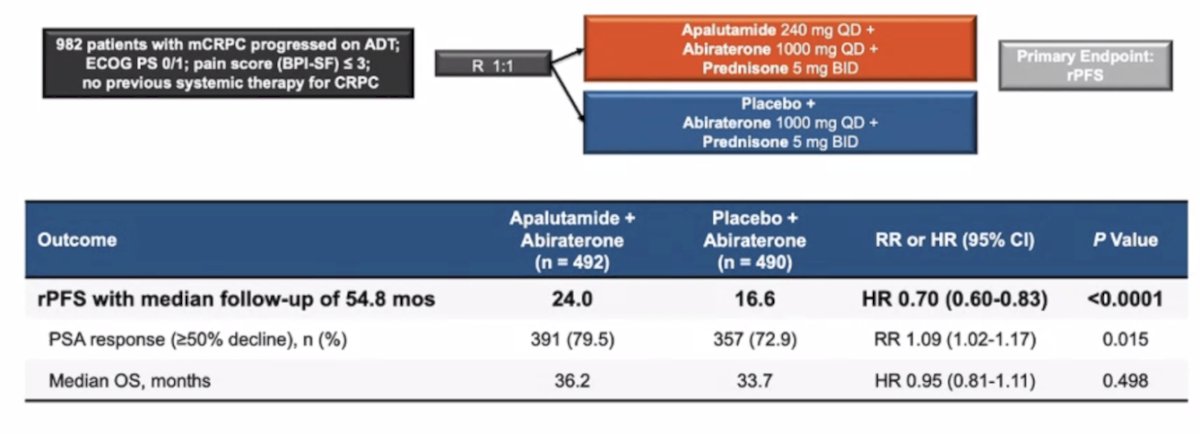
Dr. Rettig then spent some time discussing sipuleucel-T, specifically the PROCEED registry. This is a large, real-world registry of 1,902 mCRPC patients who have received >=1 sipuleucel-T infusion. One notable finding from this registry is that after a median follow-up of 46.6 months, there was a 9.5 month improvement in median overall survival for African American patients compared to Caucasian patients: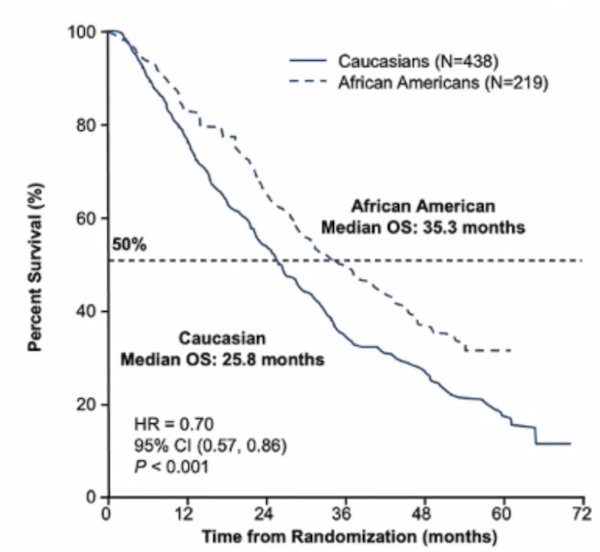
Additionally, among men with a baseline PSA < 29 ng/mL, the median overall survival was 21 months longer for African American patients versus Caucasian patients (HR 0.52, 95% CI 0.37-0.72).
To conclude his presentation, Dr. Rettig made several points regarding neuroendocrine prostate cancer as an aggressive variant. This variant arises as an adaptation to treatment, given that primary small cell prostate cancer is quite rare. It is typically AR negative/indifferent, with visceral organ and lytic bone lesion involvement, a low PSA, and associated with a short duration of ADT response. Genetic variations associated with neuroendocrine prostate cancer include p53, pRB, PTEN, MYC, AURKA, EZH2, ASCL1, FOXA2, and ONECUT2, with associated high Ki67, NSE, CGA, and synaptophysin expression. Additionally, PSMA expression is usually quite low, it may present concurrently with adenocarcinoma and is unresponsive to AR signaling inhibitors. Treatment generally is with platinum-based chemotherapy, including cisplatin + etoposide, carboplatin + etoposide, carboplatin + docetaxel, or checkpoint inhibitors (ie. atezolizumab maintenance). Treatment is generally associated with a high response rate, but short duration of response, and a median overall survival of 6-19 months. Currently, there are multiple trials for neuroendocrine prostate cancer testing novel targets to CD46, Aurora Kinase A, EZH2, and DLL3.
Presented by: Matthew Rettig, MD, UCLA, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 PSMA Conference, San Francisco, CA, Thurs, Jan 18 – Fri, Jan 19, 2024.
Related content: Treatment Landscape of mCRPC "Presentation" - Matthew Rettig
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-Repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443-453.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Chi KN, Rathkopf D, Smith MR, et al. Niraparib and abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023 Jun 20;41(18):3339-3351.
- Saad F, Efstathiou, Attard G, et al. Apalutamide plus abiraterone acetate and prednisone versus placebo plus abiraterone and prednisone in metastatic, castration-resistant prostate cancer (ACIS): A randomized, placebo-controlled, double-blind, multinational, phase 3 study. Lancet Oncol. 2021 Nov;22(11):1541-1559.