There has been significant stage migration of this disease in recent years, with a much higher percentage of stage 1 disease being diagnosed, while other stages are rising at a much lower rate. Within stage 1, there has been a decrease in the mean size of the tumors from 4.1 cm to 3.2 cm. This is explained by the increasing incidental diagnosis of these tumors, with the growing number of abdominal imaging that is performed nowadays.
Age at diagnosis of RCC is a determinant factor of cancer specific survival in patients treated with surgery, with data showing a seven-fold increase in cancer specific mortality among patients aged 75-89.1 Very similarly, data from the United Kingdom demonstrate that the mortality caused by RCC is substantially higher with over 36% over the age of 75. 2
There has also been a very substantial paradigm change in the way RCC is treated, from the initial days of Dr. Robson, who is renowned for codifying radical thoracoabdominal nephrectomy and staging of RCC, to the days of robotic partial nephrectomy, focal therapy and surveillance of small renal masses.
There is only one prospective study comparing the oncological outcomes of partial nephrectomy to radical nephrectomy. This is an European Organization for Research and Treatment of Cancer (EORTC) study (EORTC 30904) published in 2011. 3 This study clearly showed that partial and radical nephrectomy for RCC tumors deliver comparable oncological results and safety. In a meta-analysis published in European Urology journal in 2012, the evidence suggested that localized RCCs are best managed by nephron sparing procedures where technically feasible. However, the evidence base used in this met-analysis has significant limitations due to studies of low methodological quality marked by high risks of bias.
The latest European Association of Urology (EAU) guidelines on RCC recommend performing partial nephrectomy for pT1a (less than 4 cm) and pT1b (more than 4 cm but less than 7 cm). In a New England Journal of Medicine publication in 2004, an independent, graded association was demonstrated between a lower glomerular filtration rate (GFR), representing renal function, and the risk of death, cardiovascular events, and hospitalization. 4 This means that loss of renal function, resulting from the loss of renal mass due to surgery, is a major risk factor, tilting the balance towards performing partial nephrectomy instead of radical nephrectomy, whenever technically feasible. Another study had shown that partial nephrectomy compared to radical nephrectomy avoids significant renal function loss 5, as seen in figure 1.
Figure 1 – Comparison of renal function (estimated glomerular filtration rate) between partial and radical nephrectomy:
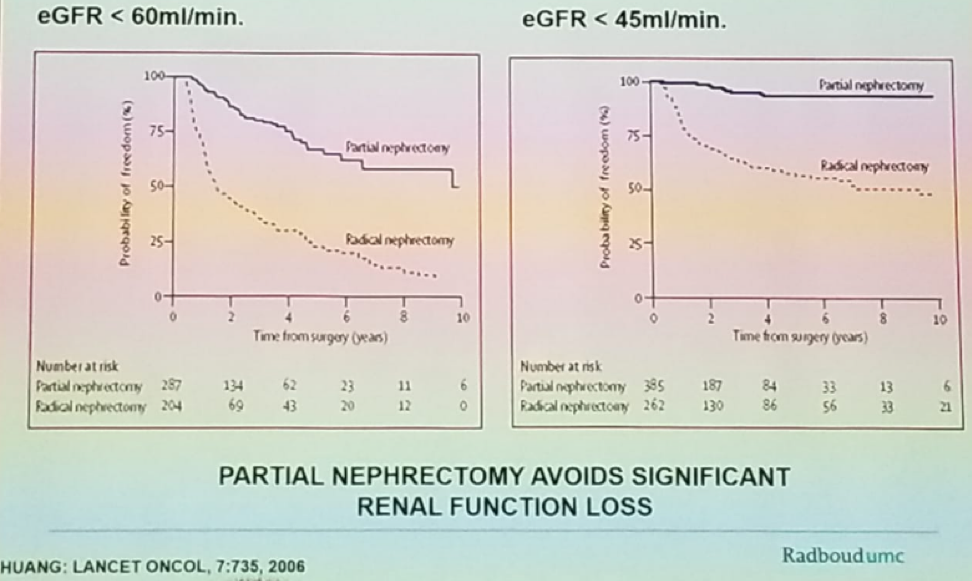
When assessing the renal function of patients who were recruited to the only randomized trial comparing partial to radical nephrectomy (EORTC 30904), it was shown that partial nephrectomy, as opposed to radical nephrectomy substantially reduced the incidence of moderate renal dysfunction (eGFR <60).6
Oncological outcomes in terms of cancer specific survival, and metastasis free survival have been shown to be identical in both open and laparoscopic partial nephrectomy.7 Data on the comparison of laparoscopic and robotic partial nephrectomy have shown that in the robotic cases the warm ischemia times were significantly shorter (19.7 vs. 284 minutes, p<0.0001).8
Surgeons always aim to reach trifecta results in partial nephrectomy, regardless of the modality being used. Trifecta results are defined as warm ischemia time less than 25 minutes, negative surgical margins, and no perioperative complications. Robotic vs. laparoscopic partial nephrectomy offers a wide range of indications, better operative outcomes, and lower perioperative morbidity. Overall the quest for trifecta appears to be better accomplished by the robotic modality, which is likely to become the new standard for minimally invasive partial nephrectomy procedure, according to Dr. Mulders.
Next, Dr. Mulders discussed the various tumor imaging scoring systems, that help surgeons standardize tumors, and understand the measure of difficulty in performing partial nephrectomy for these tumors. The two most known scoring systems are the R.E.N.A.L nephrometry score, and the PADUA score (Figure 2). These scores are derived by incorporating data on tumor location, size, endophytic component, involvement of the collecting system, and renal sinus. The PADUA score has been shown to be able to predict the risk of complication in a partial nephrectomy procedure. A PADUA score of 8-9 has a 14 times higher risk of complications, while a PADUA score of 10 or more has a 30 times higher risk of complication.
Figure 2 – The PADUA score 9:

Ficara V et al. Eur Urol 2009
Dr. Mulders moved on to discuss the factors that influence surgeons to perform partial or radical nephrectomy. Some of the known influencing factors include the patient’s age and his/her comorbidities, expert opinion and the surgeon’s own personal skills, absolute vs. relative indications for partial nephrectomy, the attachment of Gerota’s fascia, and the histology of the tumor.
Population based data has shown that increasing age tends to influence surgeons to perform radical nephrectomy rather than partial nephrectomy.10 However, there has been no difference in the 30-days mortality rate, and overall complication rate when comparing open/laparoscopic partial nephrectomy and laparoscopic radical nephrectomy in elderly patients. The only difference witnessed is a 7% higher rate of genitourinary and hemorrhagic complication rate among elderly patients.11 This leads to the fact that surgeons should not be discouraged from performing nephron sparing procedures in elderly patients, in any age, as long as their biological, and not chronological age, allows them to safely undergo this procedure.
Dr. Mulders concluded his excellent talk stating the partial nephrectomy in patients older than 75 can be performed safely and in an equal manner to that performed in younger patients. Surgeons need to have a balanced discussion with the patient and his family on the potential complications and benefit from nephron sparing procedures. The surgeon must be experienced in partial nephrectomy, disregarding the modality used (open/lap/robotic) and should be able to perform the same procedure, expecting the same oncological and functional results, whether the patient is over or under the age of 75.
Presented By: Peter Mulders, Nijmegen, The Netherlands
References:
- Karakiewicz P et al. CUAJ 2008
- Lieber et al J Urol 1981
- Van Poppel H. et al. Eur Urol 2011
- Go et al. NEJM 2004
- Huang et al. Lancet Oncol, 2006
- Scosyrev E et al. Eur Urol 2014
- Brian R et al. J Urol 2010
- Benway BM et al. Urology 2009
- Ficara V et al. Eur Urol 2009
- Russell et al. SEER database 2015
- Becker et al. Urology 2014
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre Twitter: @GoldbergHanan at the 38th Congress of the Society of International Urology - October 4- 7, 2018 - Seoul, South Korea