Athens, Greece (UroToday.com) Dr. Tilki presented on the impact of positive surgical margins, biochemical recurrence and PSA persistence on the oncological outcomes after undergoing radical prostatectomy.
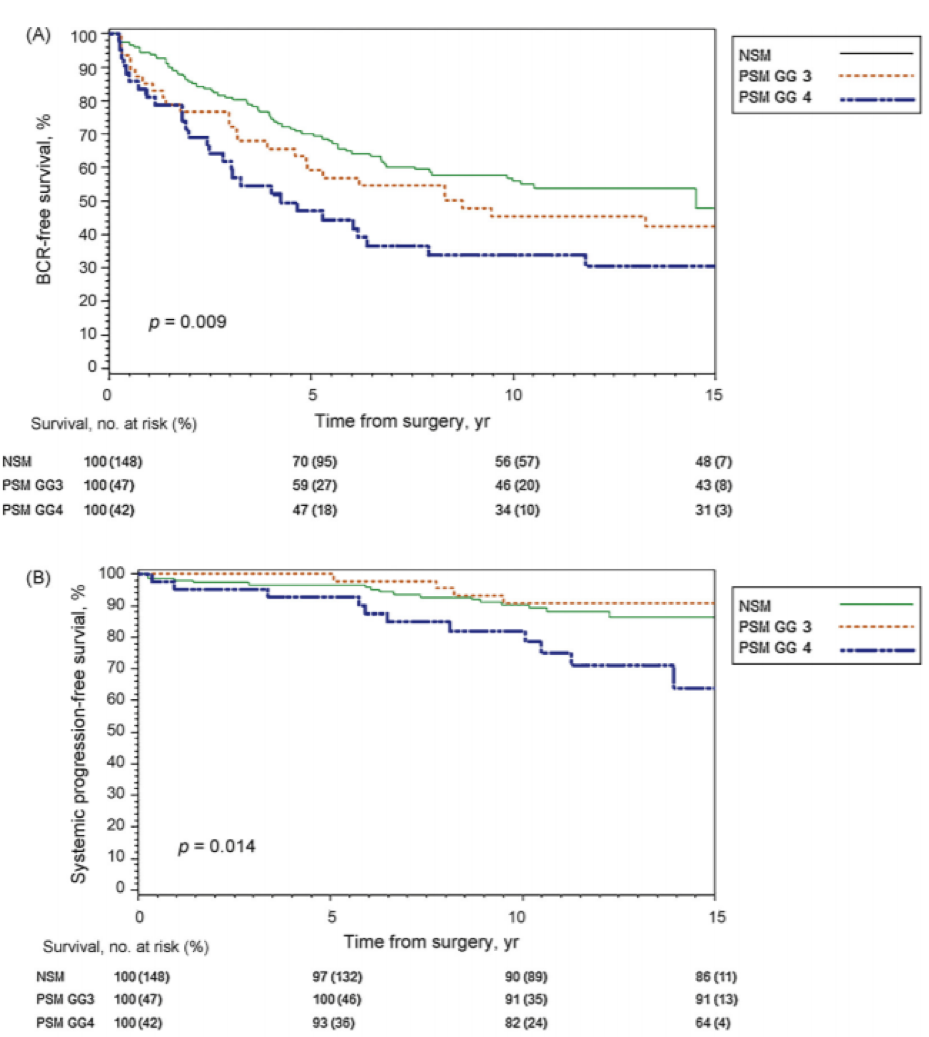
Margin status is positive if tumor cells are in contact with the ink on the specimen surface. Surgical margins are an independent risk factor for biochemical recurrence, but not all men with positive surgical margins recur and not all positive surgical margins are the same. Data from one study have shown that approximately 44% of men with positive surgical margins had no progression with a median follow-up of 13 years.1 Another study demonstrated that progression-free survival and prostate cancer-specific mortality was very different for Gleason 4 disease at the margin vs. Gleason 3 disease at the margin vs. a negative margin, as can bee seen in Figure 1.2
In another study, positive surgical margins was an independent predictor of biochemical recurrence in multivariable analysis (hazard ratio (HR) 2.4, p<0.001).3 However, in subgroups of positive surgical margins, only those positive margins longer than 3 mm represented an independent predictor (HR 1.93, p=0.04), while focality and Gleason at the margin were not shown to be significant predictors.3
Next, Dr. Tilki moved on to discuss the topic of biochemical recurrence. Biochemical recurrence continues to be reported in up to 35% of men undergoing radical prostatectomy. The natural history of biochemical recurrence after radical prostatectomy is variable and does not always translate to the systemic progression of prostate cancer death. The landmark trial by Pound et al. published in the Journal of the American Medical Association showed that metastases developed in only 304/1997 patients with elevated PSA following radical prostatectomy and with no salvage therapy.4 The median time from biochemical recurrence to metastases development was 8 years, and the median time from metastases to death was 5 years.4 Many of the men who developed biochemical recurrence remained metastasis-free for an extended period of time without any other forms of therapy. In a more recent study with a larger number of patients (14,532) following radical prostatectomy and with a median follow-up time of 50.8 months, biochemical recurrence had occurred in 20.3% of men.5
In a large systematic review assessing biochemical recurrence following radical prostatectomy, biochemical recurrence had occurred in 27-53% of patients.6 Importantly, however, only 30% of patients with biochemical recurrence after primary surgery developed clinical recurrence, with only 16% of them dying from their disease.6 The main unfavorable prognostic factors that have been incorporated into the European Association of Urology (EAU) guidelines were:
- PSA doubling time of less than 1 year
- A pathological Gleason score of 8-10
Figure 1 – Differences in progression-free survival and biochemical recurrence-free survival between different disease at the positive surgical margin2:
The last topic discussed by Dr. Tilki was persistent PSA. Approximately 5-20% of men continue to have detectable or persistent PSA following radical prostatectomy (>0.1 ng/ml) within 4-8 weeks of surgery.7 There are several potential reasons for this:
- Persistent local disease
- Pre-existing metastatic disease
- Residual benign prostate tissue
Data from a long-term follow-up of 15 years after radical prostatectomy showed that the metastasis-free survival and cancer-specific survival was 53% vs. 93.2% (p<0.001) and 75.5% vs. 96.2%, (p<0.001) for patients with a persistent vs. undetectable PSA, respectively.7 In a multivariable analysis, the following variables were shown to be independently associated with an increased risk for persistent PSA (all p<0.01) included:
- Higher preoperative PSA
- More advanced pathologic tumor stage
- Gleason group 3-5
- Positive surgical margins
- Positive pelvic lymph nodes
Currently, the EAU guidelines recommend performing a PSMA pet scan when the PSA rises above 0.2 ng/ml after surgery. Moreover, treatment is recommended with salvage radiotherapy and hormonal therapy.
Concluding her talk, Dr. Tilki summarized that not all men with positive surgical margins recur. Additionally, not all biochemical recurrence progress to clinical recurrence or cancer death. Lastly, persistent PSA after radical prostatectomy is associated with more advanced disease and poor prognosis. These patients may benefit from early aggressive multi-modal treatment.
Presented by: Derya Tilki, MD, Attending Urologist, Martini-Klinik Prostate Cancer Center, University Hospital Hamburg-Eppendorf, Hamburg, Germany
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New York, USA, Twitter: @GoldbergHanan at the 39th Congress of the Société Internationale d'Urologie, SIU 2019, #SIUWorld #SIU2019, October 17-20, 2019, Athens, Greece
References:
4. Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. Jama 1999; 281(17): 1591-7.