This discussion focused on high-intensity focused ultrasound (HIFU) modality. This entails ultrasound waves delivered transrectally from a spherical transducer. The high-intensity waves converge to a focal point and cause hyperthermia and damage to the tissue. The mechanism of action consists of three effects:
- Thermal effect – focal thermal induction and rapid rise in temperature (>80 Celsius)
- Mechanical effect - generation of gas bubbles, collapse of cavities, and rupture of cell walls
- Tissue effect – coagulation necrosis which occurs immediately, an inflammatory response, which occurs after 7 days, and an induction of fibrosis, which occurs after 14 days
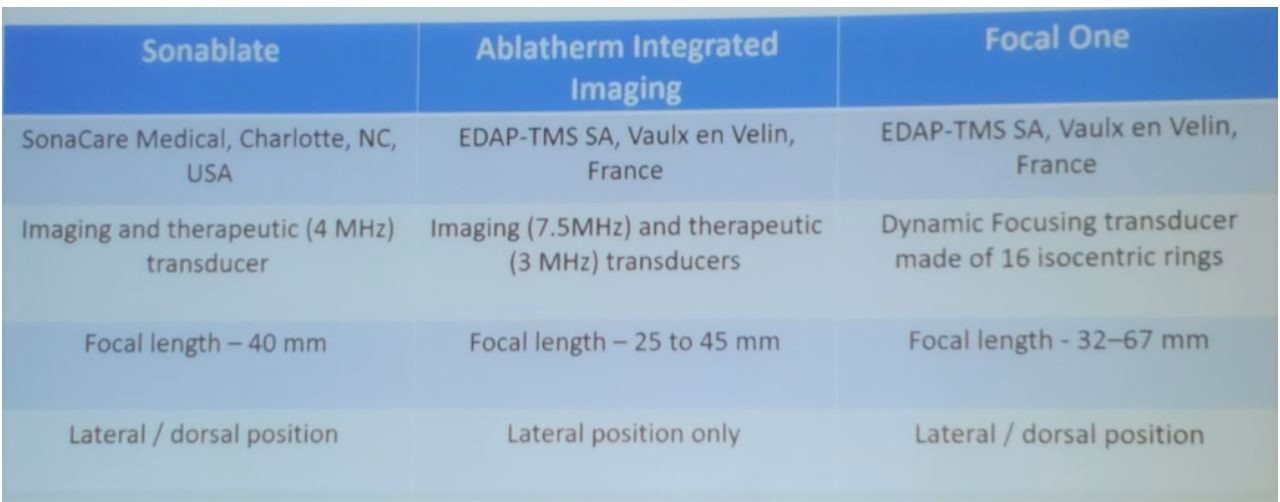
Table 1 – HIFU devices:
HIFU enables to fuse the images of the mpMRI together with the ultrasound images to create an elastic fusion, making the tumor now visible on the ultrasound image. The goal of HIFU, with its ability to fuse tumor images, is to treat the index lesion with the most aggressive cancer. The limitations of this technique are in defining the actual size and borders of the significant index lesion that is going to be treated. It greatly depends on the expertise of the radiologists interpreting the mpMRI images, and any ablation performed should account for a reasonable security margin. Another important limitation is treating apical tumors. Apical tumors can only be treated with HIFU if the ultrasound images allow to distinguish prostate tissue from the sphincter.
Dr. Vallancien described a study showing his own experience with hemiablation using HIFU in 12 patients with 10-year follow-up.2 The relapse free survival was 90% at 5 years, and 38% at 10 years. Five patients had salvage HIFU therapy or hormone therapy and all patients were alive at 10 years.
The next topic discussed was the complication rate in HIFU treatment. In a comprehensive evaluation of this treatment modality 98 complications had occurred in 79 / 210 patients (37.6%). 94.9% of the complications were Clavien-Dindo grade 1-2. Most complications occurred within 30 days of treatment (84.7%), and the readmission rate was 5.7%.
Next, Dr. Vallancien gave some data on the comparison between focal therapy and robotic radical prostatectomy (RALP).3 The biochemical recurrence rate was 6.1% in RARP vs. 9% in focal therapy (but the criteria that were used were different for each modality…). The failure rate on focal therapy was 28.8%. The need for salvage therapy was 13.8% and 23% at 20 months and 46 months in patients treated with focal therapy.
Dr. Vallancien presented his center’s experience with focal therapy with very high failure free survival rates, as can be seen in Table 2. The main predictors of failure following focal therapy were Gleason score >=3+4, more than 15% cores positive in the biopsy, and a PSA nadir >=2.5 ng/ml.
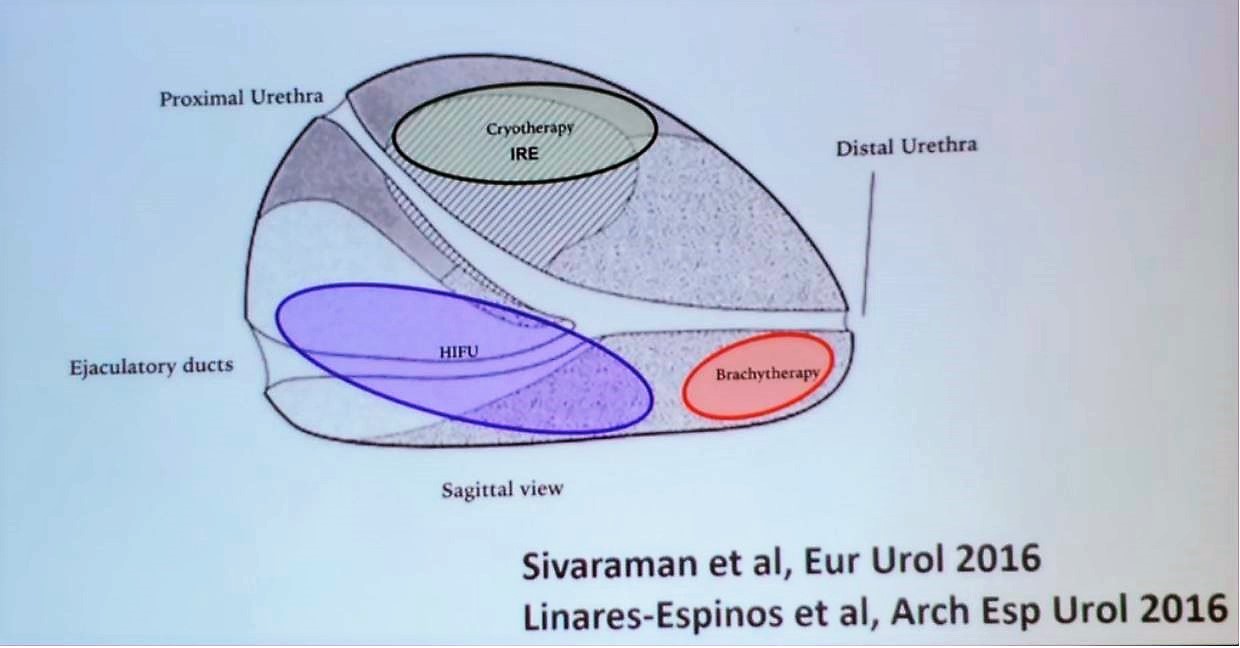
Due to the various attributes, advantages, and disadvantages of each focal therapy modality, there is a recommendation to perform different focal therapy techniques according to the location of the tumor,4 as can be seen in Figure 1. According to expert consensus, posterior lesions are better amenable to HIFU, while cryotherapy provides the best possible outcomes for anterior tumors, and apical lesions need to be treated with focal brachytherapy. Using these recommendations side effects will be low, urinary continence rates will be above 90% and erectile dysfunction between 5-52%.
Table 2 – Institute Montsouris Paris, France focal therapy experience:
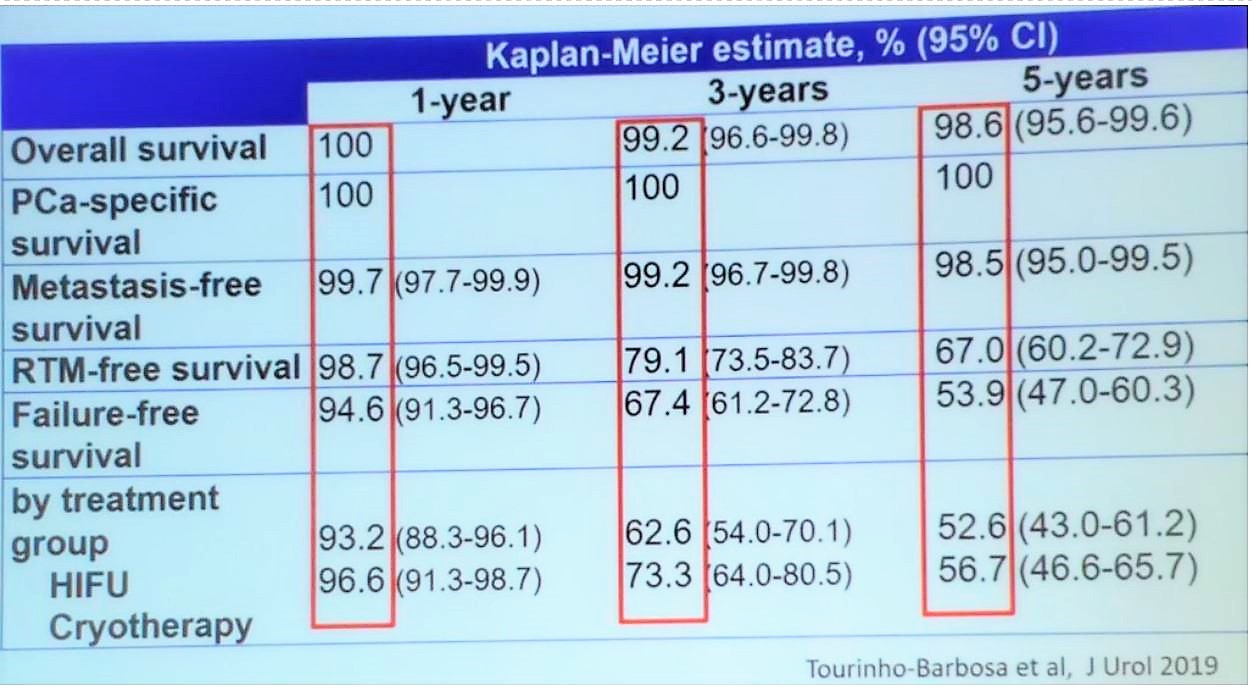
Figure 1 – Which focal therapy to use according to the prostate tumor location:
Summarizing his talk, Dr. Vallancien stated that we are still lacking long-term cancer control data with focal therapy, and the outcomes need to be improved. Focal therapy represents a promising alternative to treat intermediate-risk disease of Gleason 3+4, or low-risk tumors without an indication for active surveillance. In selected patients, hemiablation combined with mpMRI represents an accurate treatment option of the index lesion.
Figure 1 – Which focal therapy to use according to the prostate tumor location:
Summarizing his talk, Dr. Vallancien stated that we are still lacking long-term cancer control data with focal therapy, and the outcomes need to be improved. Focal therapy represents a promising alternative to treat intermediate-risk disease of Gleason 3+4, or low-risk tumors without an indication for active surveillance. In selected patients, hemiablation combined with mpMRI represents an accurate treatment option of the index lesion.
Presented by: Guy Vallancien, MD, Institute Montsouris, University of Paris, Paris, France
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New York, USA, Twitter: @GoldbergHanan at the 39th Congress of the Société Internationale d'Urologie, SIU 2019, #SIUWorld #SIU2019, October 17-20, 2019, Athens, Greece
References:
1. Barret E, Ahallal Y, Sanchez-Salas R, et al. Morbidity of Focal Therapy in the Treatment of Localized Prostate Cancer. European Urology 2013; 63(4): 618-22.
2. El Fegoun AB, Barret E, Prapotnich D, et al. Focal therapy with high-intensity focused ultrasound for prostate cancer in the elderly. A feasibility study with 10 years follow-up. International braz j urol : official journal of the Brazilian Society of Urology 2011; 37(2): 213-9; discussion 20-2.
3. Garcia-Barreras S, Sanchez-Salas R, Sivaraman A, et al. Comparative Analysis of Partial Gland Ablation and Radical Prostatectomy to Treat Low and Intermediate Risk Prostate Cancer: Oncologic and Functional Outcomes. Journal of Urology 2018; 199(1): 140-6.
4.Ganzer R, Arthanareeswaran VKA. Which technology to select for primary focal treatment of prostate cancer?-European Section of Urotechnology (ESUT) position statement. 2018; 21(2): 175-86.
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New York, USA, Twitter: @GoldbergHanan at the 39th Congress of the Société Internationale d'Urologie, SIU 2019, #SIUWorld #SIU2019, October 17-20, 2019, Athens, Greece
References:
1. Barret E, Ahallal Y, Sanchez-Salas R, et al. Morbidity of Focal Therapy in the Treatment of Localized Prostate Cancer. European Urology 2013; 63(4): 618-22.
2. El Fegoun AB, Barret E, Prapotnich D, et al. Focal therapy with high-intensity focused ultrasound for prostate cancer in the elderly. A feasibility study with 10 years follow-up. International braz j urol : official journal of the Brazilian Society of Urology 2011; 37(2): 213-9; discussion 20-2.
3. Garcia-Barreras S, Sanchez-Salas R, Sivaraman A, et al. Comparative Analysis of Partial Gland Ablation and Radical Prostatectomy to Treat Low and Intermediate Risk Prostate Cancer: Oncologic and Functional Outcomes. Journal of Urology 2018; 199(1): 140-6.
4.Ganzer R, Arthanareeswaran VKA. Which technology to select for primary focal treatment of prostate cancer?-European Section of Urotechnology (ESUT) position statement. 2018; 21(2): 175-86.