(UroToday.com) The 2024 Society of Nuclear Medicine & Molecular Imaging (SNMMI) annual meeting featured a session on prostate cancer, and a presentation by Dr. Tao Sun discussing the simplified quantification method of [18F]AlF-P16-093 for patients with primary prostate cancer. This work presents the optimization of pharmacokinetic modeling for a new tracer, [18F]AlF-P16-093, for in-vivo prostate cancer imaging.
[18F]AlF-P16-093 is a PSMA radiopharmaceutical that is automatically synthesized with a GE TRACERlab™, with few metabolites, and no reportable side-effects. PSMA-positive tumors display rapid uptake and are all detectable in 10 minutes after injection. The alternate simplified quantification approach for full dynamic imaging was also investigated to facilitate its clinical translation.
Dynamic PET/CT scans were conducted on eight patients with primary prostate cancer, followed by a whole-body PET scan 60 minutes post-injection. The characteristics of these patients are as follows: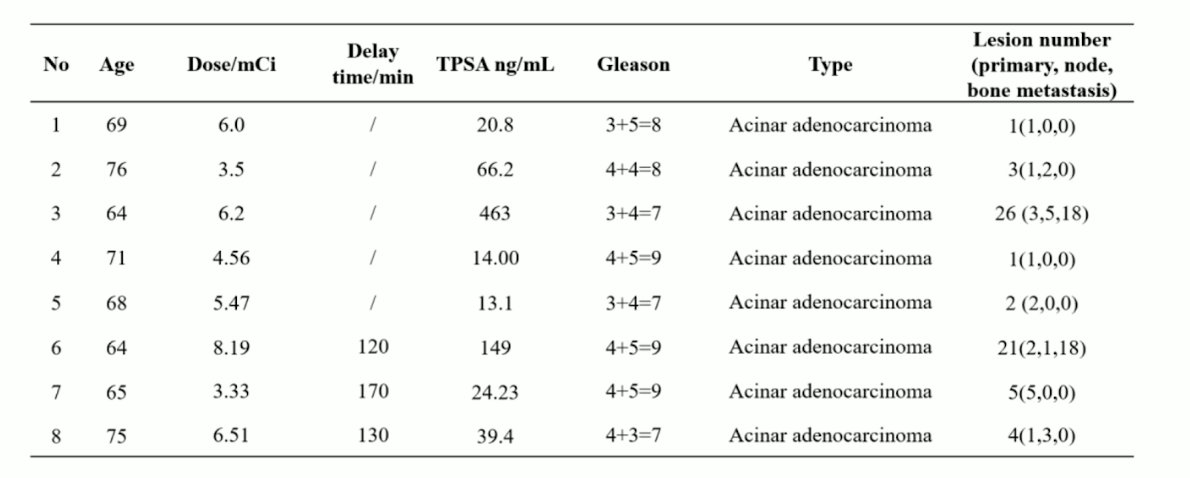
An example of dynamic imaging is below for a 64-year-old with Gleason 4+5 = 9 prostate adenocarcinoma and a PSA of 149 ng/mL:
Time-activity curves were produced by delineating volumes of interest for primary prostatic and metastatic lesions. Intraprostatic, lymph node and osseous metastases increased sharply at the beginning 60 seconds post-injection, then increased moderately until 30 minutes. All tumors reached a plateau uptake in the following 30-60 minutes, and the bladder began to accumulate slowly after 4 minutes post-injection and was higher than the uptake intraprostatic after 10 minutes: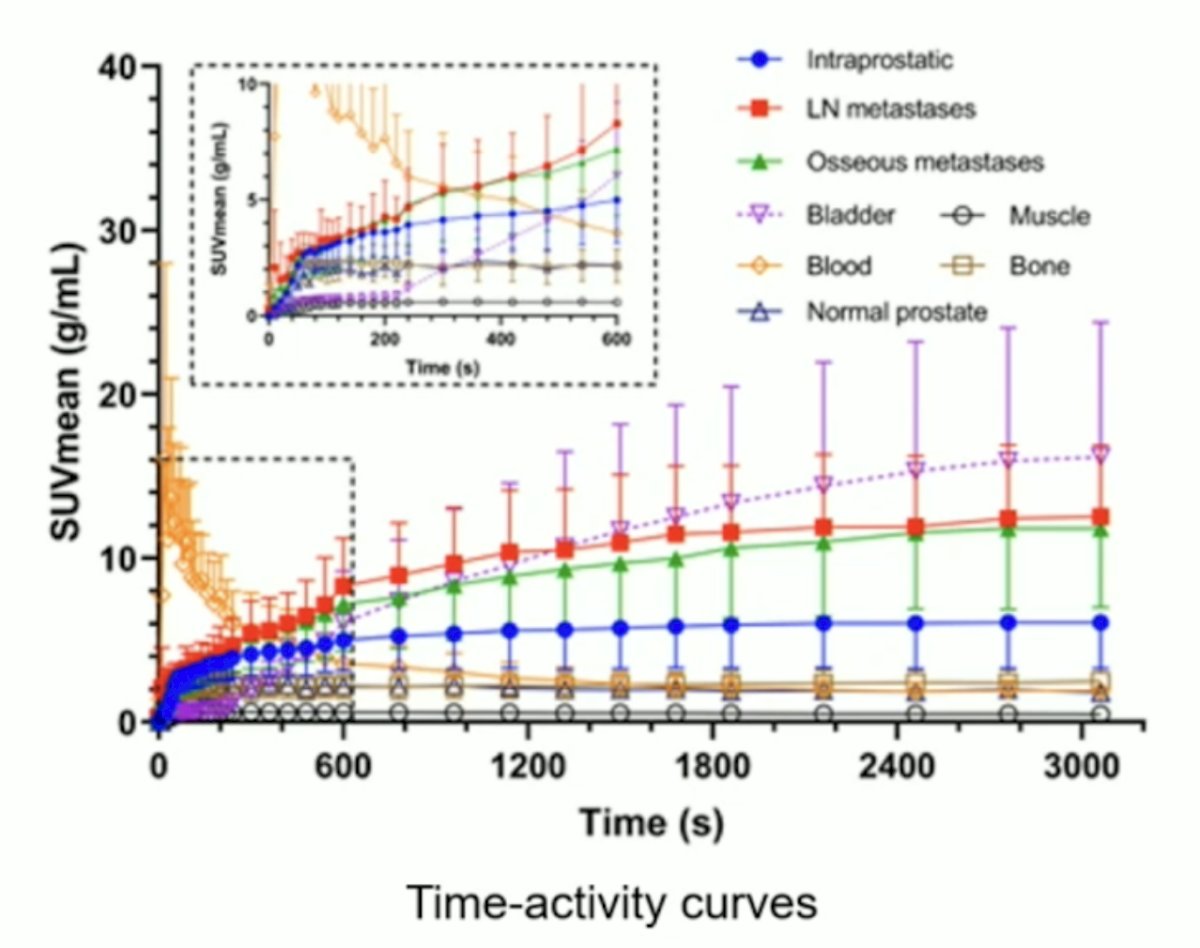
Optimal kinetic modeling was evaluated under the assumption of three candidate compartmental models (1T2K, 2T3K, and 2T4K) with accounting for fractional blood volume. The image-derived input function was extracted by applying the abdominal aorta mask to each dynamic frame. The simplified quantification approach was then derived based on the association between the static uptake measure and total distribution volume computed based on the selected model.
In total, 17 intraprostatic lesions, 10 lymph nodes, and 36 osseous metastases were investigated. Visually, the contrast to background of the tumor arose and showed the steepest slope within the first few minutes while background activity diminished over time. Full pharmacokinetic investigation found that a reversible two-compartmental (2T4K) model is the preferred model for the provided tracer: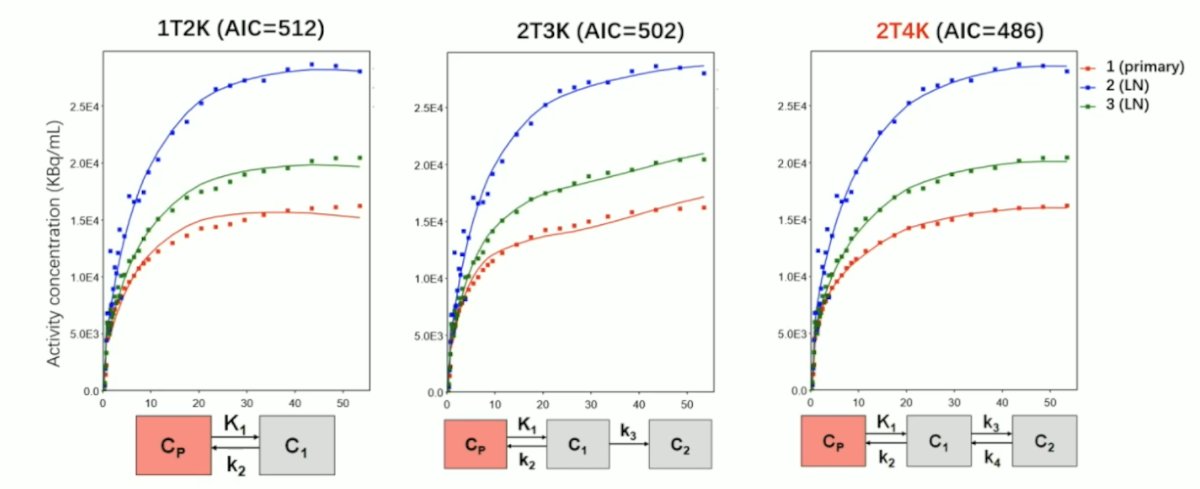
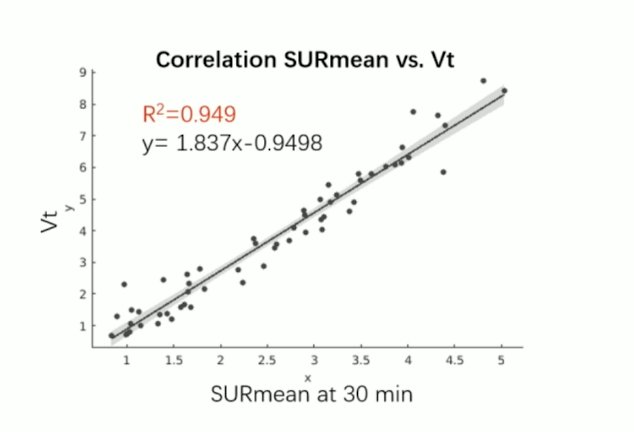
The kinetic parameters K1, K3, blood volume, and distribution volume were considerably greater in lesions than normal tissue (p < 0.01). Several simplified quantification methods were tested for approximating full dynamic quantification in lesions, with image-based SURmean (the ratio of tumor SUVmean to blood SUVmean) within the 28-34 min window shown to be sufficient for estimating the total distribution volume values (R2 = 0.949, p < 0.01):
Finally, both the distribution volume and SURmean after 30 mins were associated strongly with the total serum PSA levels (p < 0.01). The PSA correlations are as follows:
- Vt vs PSA: rho = 0.527, p < 0.001
- SUR30 vs PSA: rho = 0.421, p = 0.001
- Vt vs Gleason: rho 0.128, p = 0.675
- SUR30 vs Gleason: rho 0.214, p = 0.483
Dr. Sun concluded this presentation discussing the simplified quantification method of [18F]AlF-P16-093 for patients with primary prostate cancer with the following take-home messages:
- This study introduced an optimized pharmacokinetic modeling approach and a simplified acquisition method for [18F]AlF-P16-093
- This highlights the feasibility of utilizing one static window (after 30 minutes) for diagnosis of prostate cancer
- Patient number is limited as the dynamic scan is difficult for the patients to endure over 30 minutes
- Patient body movement can result in severe misplacements of the vessel ROI required for IDIF extraction, which is used instead of arterial blood sampling
- This methodology requires clinical validation
Presented by: Tao Sun, PhD, Associate Professor, Shenzhen Institute of Advanced Technology, Guangdong, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 Society of Nuclear Medicine & Molecular Imaging (SNMMI) Annual Meeting, Toronto, Ontario, Canada, Sat, June 8 – Tues, June 11, 2024.