Sacral is the Target
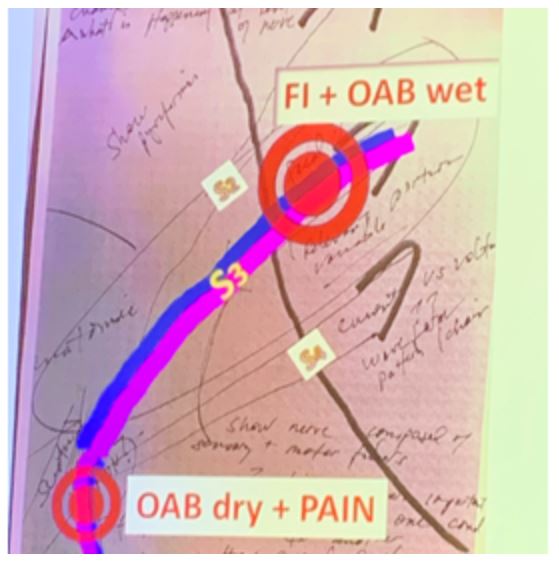
Dr. Steven Siegel covers the Sacral is the Target presentation topic in this Point-Counterpoint presentation. He starts by explaining general goals for neuromodulation which are to ensure the lead tracks along the natural nerve path, keeping 4/4 leads < 2mA and observing the appropriate pattern of motor and sensory responses. He debates the response for sacral neuromodulation and tibial lead may not have the same response. He discusses anatomy and the nerve paths and how the S3 nerve may have different targets depending on the patient’s symptoms.
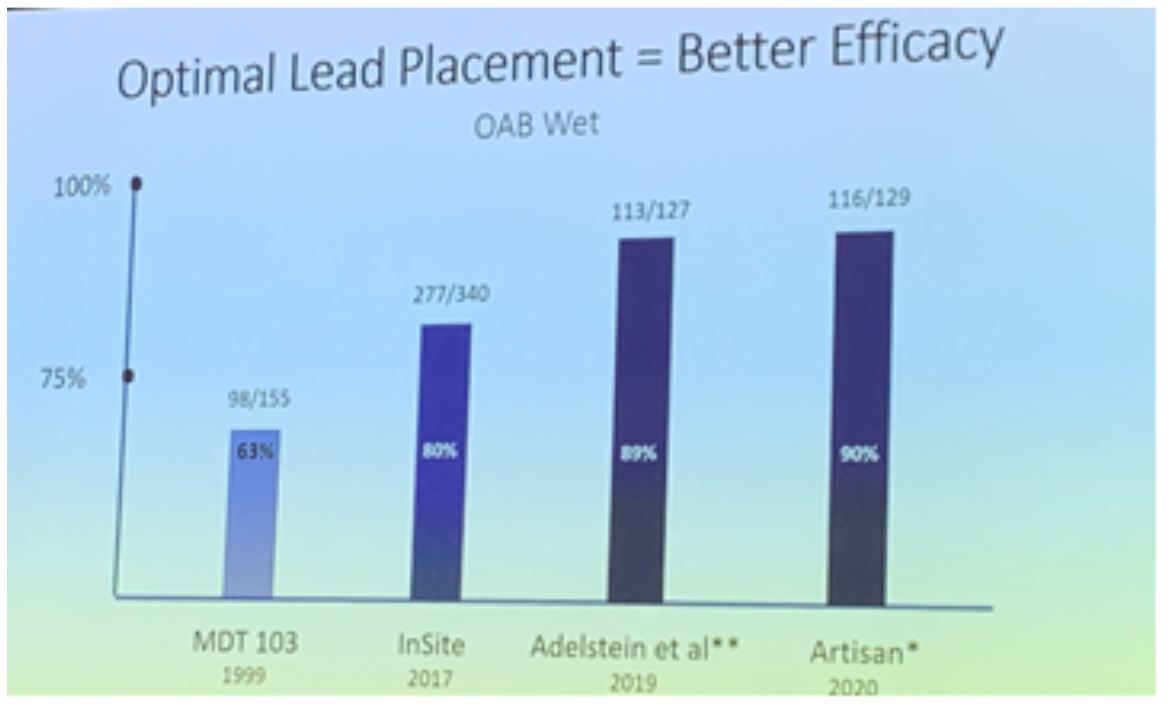
He mentions all the areas for future research: type of stimulation, pulse, chains of stimulation … a lot of potential to leverage networks of nerves and specific targets. Optimal lead placement improves efficacy, which is demonstrated over time with several studies.
Dr. Siegel mentions his views that an implantable lead or another target may be attractive however the following should be true: results should be similar to sacral neuromodulation, the procedure should be able to be done by the same provider, review if the benefit is worth the risk and patient needs to want it.
He concludes his debate with the next generation of sacral neuromodulation which has some clear advantages.

Other Targets
Dr. Scott MacDiarmid begins his discussion with his objective which includes speaking to a clinical problem, sacral neuromodulation (SNM) is not for the masses and shine a light on other targets. He the refractory overactive bladder patient, otherwise known as “ROAB”. He reviews the AUA guideline definitions and management of ROAB patients. There are however many different types of refractory OAB patients with different presentations who may not find benefit in the treatment algorithm defined. He mentions several reasons why sacral neuromodulation may not be performed: apathy, perceived invasiveness, durability/revision, cost, patient types (older/frail), awareness, conditional MRI (which is no longer a limitation due to new product on market).
He states that the current treatment algorithm needs more targets! As of now, PTNS is available and minimally invasive with good data. The Sumit trial by Peters reports good data that mirrors clinical practice. The STEP study showed durability in the ankle is consistent and does not seem to fade. Is this due to neuroplasticity?? Why PTNS vs SNM? It is minimally invasive, cost-effective, no safety concerns, often the only option for the patient. He asks, can PTNS become an approach to neuromodulation for the masses? …. But barriers still exist. He introduces eCoin™ which is the size of a nickel, 23 mm diameter, 2.2 mm thick. There is a prospective, single-arm study that is ongoing. This is an office-based procedure with feasible data, well tolerated with minimal adverse events.

This addresses primary barriers to current ROAB therapies, including retreatment PTNS, fear of retention with botulinum toxin and perceived invasiveness of SNM. He concludes by discussing the future target, saphenous nerve. He showed his study by placing a PTNS needle along the saphenous nerve. The nerve is so superficial can do transcutaneously and showed a future development. All in all, the treatment goal is to be patient-centric because all patients are different.

Presented by:
Moderator: Cristiano Gomes, MD, PhD, Associate Professor of Urology, University of Sao Paulo School of Medicine, Brazil
Sacral is the Target - Steven W. Siegel, MD, Director, Metro Urology Centers for Female Urology and Continence Care, St. Paul, Minnesota
Other Targets - Scott A. MacDiarmid, MD, Director, Alliance Urology Specialists Bladder Control and Pelvic Pain Center Moses H. Cone Memorial Hospital, Greensboro, North Carolina
Written by: Lira Chowdhury, DO, Urology Specialist, Urology Partners of North Texas, PLLC, Fort Worth, Texas at the Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction Winter Meeting, SUFU 2020, February 25 - February 29, 2020, Scottsdale, Arizona
He mentions all the areas for future research: type of stimulation, pulse, chains of stimulation … a lot of potential to leverage networks of nerves and specific targets. Optimal lead placement improves efficacy, which is demonstrated over time with several studies.
Dr. Siegel mentions his views that an implantable lead or another target may be attractive however the following should be true: results should be similar to sacral neuromodulation, the procedure should be able to be done by the same provider, review if the benefit is worth the risk and patient needs to want it.
He concludes his debate with the next generation of sacral neuromodulation which has some clear advantages.
Other Targets
Dr. Scott MacDiarmid begins his discussion with his objective which includes speaking to a clinical problem, sacral neuromodulation (SNM) is not for the masses and shine a light on other targets. He the refractory overactive bladder patient, otherwise known as “ROAB”. He reviews the AUA guideline definitions and management of ROAB patients. There are however many different types of refractory OAB patients with different presentations who may not find benefit in the treatment algorithm defined. He mentions several reasons why sacral neuromodulation may not be performed: apathy, perceived invasiveness, durability/revision, cost, patient types (older/frail), awareness, conditional MRI (which is no longer a limitation due to new product on market).
He states that the current treatment algorithm needs more targets! As of now, PTNS is available and minimally invasive with good data. The Sumit trial by Peters reports good data that mirrors clinical practice. The STEP study showed durability in the ankle is consistent and does not seem to fade. Is this due to neuroplasticity?? Why PTNS vs SNM? It is minimally invasive, cost-effective, no safety concerns, often the only option for the patient. He asks, can PTNS become an approach to neuromodulation for the masses? …. But barriers still exist. He introduces eCoin™ which is the size of a nickel, 23 mm diameter, 2.2 mm thick. There is a prospective, single-arm study that is ongoing. This is an office-based procedure with feasible data, well tolerated with minimal adverse events.
This addresses primary barriers to current ROAB therapies, including retreatment PTNS, fear of retention with botulinum toxin and perceived invasiveness of SNM. He concludes by discussing the future target, saphenous nerve. He showed his study by placing a PTNS needle along the saphenous nerve. The nerve is so superficial can do transcutaneously and showed a future development. All in all, the treatment goal is to be patient-centric because all patients are different.
Presented by:
Moderator: Cristiano Gomes, MD, PhD, Associate Professor of Urology, University of Sao Paulo School of Medicine, Brazil
Sacral is the Target - Steven W. Siegel, MD, Director, Metro Urology Centers for Female Urology and Continence Care, St. Paul, Minnesota
Other Targets - Scott A. MacDiarmid, MD, Director, Alliance Urology Specialists Bladder Control and Pelvic Pain Center Moses H. Cone Memorial Hospital, Greensboro, North Carolina
Written by: Lira Chowdhury, DO, Urology Specialist, Urology Partners of North Texas, PLLC, Fort Worth, Texas at the Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction Winter Meeting, SUFU 2020, February 25 - February 29, 2020, Scottsdale, Arizona