The management of testicular cancer changed drastically with the introduction of cisplatin therapy in the 1970’s by Dr. Einhorn. Since its introduction, cisplatin has now become a mainstay of systemic therapy for multiple malignancies – it is now the most commonly used group of cytotoxic drugs worldwide! However, studies have demonstrated persistent serum and urine levels up to 20 years after initial treatment.
Testicular cancer affects primarily men between the ages of 18 and 35, and now carries survival rates exceeding 95%. As such, these men often gain ~40 years of life with systemic therapy. Testicular cancer survivors now account for 4% of male cancer survivors. During that lifetime, they are at increased risk of acute and late effects of testicular cancer and its therapies.
Cisplatin has some known, acknowledged toxicities:
1) Ototoxicity – permanent bilateral hearing loss, tinnitus
- One of the most ototoxic drugs in clinical use
- 500,000 new cancer patients each year develop ototoxicity
- Little data re: genetic variants and susceptibility
- TPMT and COMT mutations: 7-21X increased risk
- One of the most common and potentially permanent side effects
- Significant impact on QOL
- Few preventative measures
- 9 major TCa centers are participating
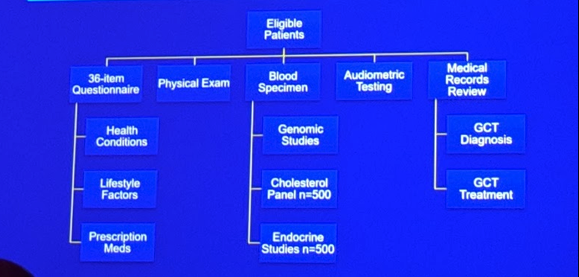
- Eligibility criteria:
- Age < 55 with GCT
- First-line cisplatin-based chemotherapy
- No subsequent salvage therapy
- Routine follow-up at the treatment site
She then spent most of the rest of the talk providing some early data and results. Below, I highlight some of the key points:
Demographics – 952 patients accrued so far.
- Median age 37 years
- Primarily white (86%) and well-educated (87% at least college degree)
- 59% BEP or 32% EP
- Median time from cisplatin therapy: 4.7 years
- Significant relationship between cisplatin dose and hearing loss at different Hz levels
- 1 in 5 patients had “severe” (by ASHA standards) hearing loss!
- There are some early GWAS results that suggest certain associations to hearing loss predilection
- Rs62283056 – each minor allele increased hearing loss 2.3X fold in patients given >300 mg/m2 cisplatin than in patients given lower doses
- Did NOT replicate SNPs identified in prior studies
- Predominantly large fiber sensory neuropathy loss
- Symptom assessment was either by physician grading and/or validated, patient reported outcomes (preferred)
- 54% of patients reported neuropathy
- Age, excess drinking, smoking, HTN increased risk
- Genetics results reported – highly polygenic!
- Prior study SNPs not replicated
- Associated with lower expression of RPRD1B
- Besides the above, others included Raynaud’s (18.7% - but 28.8% after BEP x 4), Obesity (31%), HTN on medication (11.6%), HLP on medications (10.6%), hypogonadism on testosterone (9.9%), psychotropic medication (10.4%)
- When comparing regimens (BEP vs EP), no difference in overall # of adverse events
- Self-reported health decreased as AHO’s increased
- Few studies accounting for number&severity of adverse events in survivors
- In this study, they mapped all the health outcomes to CTCAEv4 and graded them
- This is what they found:

- 70% had low-medium cumulative burden
- 20% had high, very high or severe burden
- Older age at evaluation, < college education, on disability leave, and current/former smokers were at higher risk of greater cumulative burden of morbidity
Presented By: Lois B. Travis, MD, ScD
Written by: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University, @tchandra_uromd, @TjuUrology, at the 19th Annual Meeting of the Society of Urologic Oncology (SUO), November 28-30, 2018 – Phoenix, Arizona