Washington, DC (UroToday.com) Non-muscle invasive bladder cancer (NMIBC) has high rates of recurrence and low risk of progression. However, the natural history of NMIBC is heterogeneous, with significant variation depending on stage and grade at diagnosis. Currently, available risk calculators provide broad estimates of any recurrence and progression to muscle-invasive disease but are not able to predict the stage and grade of the recurrence. Understanding the patterns of recurrence on a more granular level may enable risk-stratified NMIBC treatment and surveillance. At the 20th Annual Meeting of the Society of Urologic Oncology, during the Young Urologic Oncologists Podium Session, Dr. Tullika Garg presented her study titled Risk of Multiple Levels of Recurrence and Progression after Initial Diagnosis of Non-Muscle Invasive Bladder Cancer in a Multi-Site, Community-Based Cohort. The study aimed to predict the risk of multiple levels of recurrence and progression outcomes across the NMIBC stage and grade in a large cohort from two community-based health systems- Geisinger and Kaiser Permanente Northwest (KPNW).
Dr. Garg then described the design of this study. The analysis cohort consisted of 2956 NMIBC (stage <T2) patients from the two centers diagnosed between 1994-2015. Data were derived from tumor registries, electronic health records, membership files, and pathology records. Recurrences (n=1062) were identified using a computer algorithm, and all pathology reports were annotated for stage and grade by two urologic oncologists. Initial NMIBC diagnosis as a composite stage and grade variable were defined as a papillary urothelial neoplasm of low malignant potential (PUNLMP), Ta low grade, Ta high grade, Tis or Ta with carcinoma in situ (CIS), T1 low grade, and T1 high grade. Recurrences were defined as low risk (PUNLMP or Ta low grade), intermediate-risk (Ta high grade, CIS, T1 low grade), or high risk (T1 high grade), or progression to muscle invasion. Four outcomes were defined as any recurrence, intermediate-risk recurrence or higher, high-risk recurrence or higher, and progression to muscle invasion. Separate Cox proportional hazards regressions were performed to determine the association between each initial stage/grade category and time to each ordered outcome. Multivariable models were adjusted for age, sex, health system (KPNW or Geisinger), initial tumor size (<3cm or >=3cm), the initial number of tumors (unifocal vs. multifocal), perioperative intravesical chemotherapy (yes/no), and induction intravesical therapy (yes/no). 1- and 5-year risk estimates were computed, and 95% confidence intervals (CI) were associated based on these models.
Dr. Garg then presented the results of this study. The mean age at diagnosis was 69 years, and the cohort was predominantly white (98.5%), male (79%), and from KPNW (66%). At initial diagnosis, nearly half (1420) of tumors were Ta low grade, 78% were unifocal, and 77% were less than 3cm in size. Over a median follow up of 29.4 months, there were 1062 recurrences (35.9% of the cohort), and a total of 111 patients had progression to muscle-invasion (3.8%). PUNLMP was associated with a decreased risk of any recurrence as compared to Ta low grade (adjusted HR 0.72, 95% CI 0.56-0.92). The adjusted hazard of high-risk recurrence (T1 high grade) or progression increased with increasing diagnosis stage/grade from Ta high grade (adjusted HR 2.60, 95% CI 1.62-4.15), Tis or Ta with CIS (adjusted HR 4.74, 95% CI 3.01-7.47), and T1 high grade (adjusted HR 7.14, 95% CI 4.97-10.26). Figures below are the screenshots from the slides presented, showing the predicted 1- and 5-year risks of each outcome by stage and grade at diagnosis.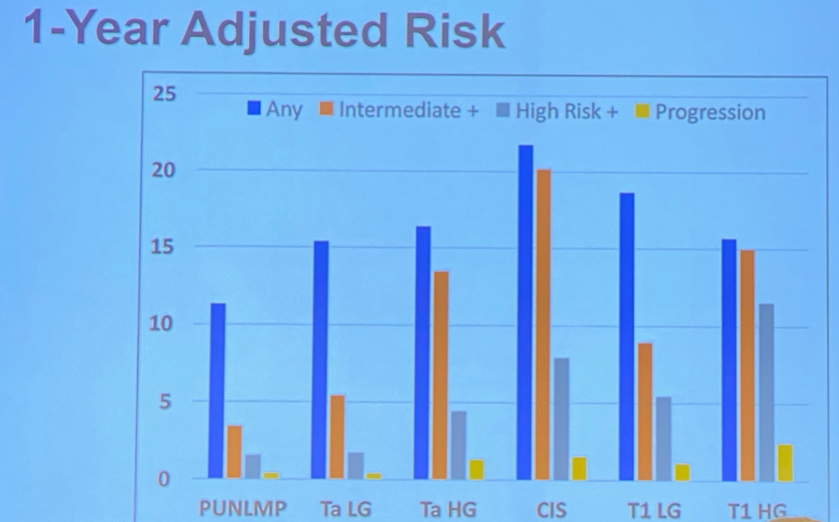
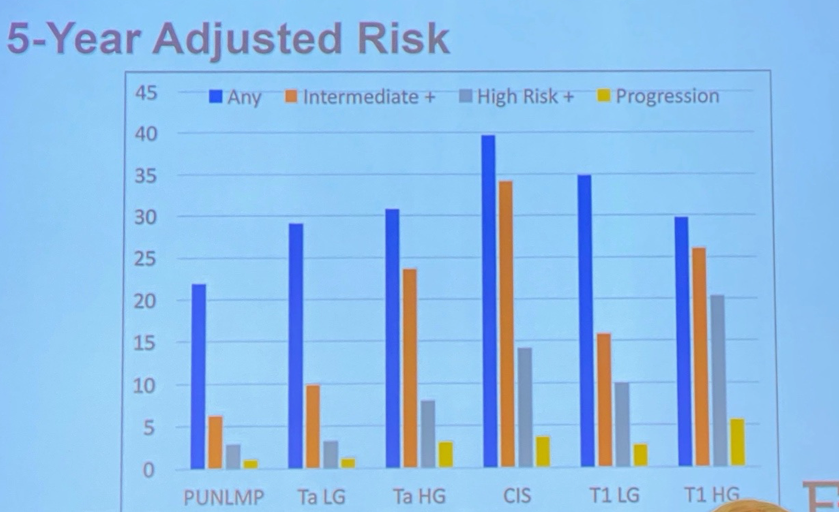
Lastly, Dr. Garg presented the conclusion of this large study of NMIBC patients from two community-based health systems. This is one of the largest existing series of long-term PUNLMP outcomes. 1- and 5- year predicted risk of high-risk recurrences (T1 high grade) and progression to muscle-invasive disease increased with higher composite stage and grade at diagnosis. The predicted risks of multilevel NMIBC recurrence and progression outcomes may be useful for counseling patients and for designing risk-stratified surveillance schedules.
Presented by: Tullika Garg, MD, MPH, Urologic Oncologist and Health Services Researcher, Department of Urology, Geisinger, Danville, Pennslyvania, USA.
Written by: Abhishek Srivastava, MD, Society of Urologic Oncology Fellow, Fox Chase Cancer Center, Fox Chase Cancer Center, Philadelphia, PA at the 20th Annual Meeting of the Society of Urologic Oncology 2019. Twitter: @shekabhishek at the 20th Annual Meeting of the Society of Urologic Oncology (SUO), December 4 - 6, 2019, Washington, DC