(UroToday.com) The 2024 SUO annual meeting included a Keynote Lecture by Dr. Gopa Iyer discussing FGFR and precision in urothelial carcinoma. Dr. Iyer notes that FGFR binding to FGF ligands leads to dimerization of FGF receptors. This subsequently leads to downstream signaling through MAPK and PI3K/Akt pathways, resulting in promotion of cell survival, upregulation of cell growth, and division.
With regards to FGFR inhibition in cancer, erdafitinib is a pan-FGFR TKI (FGFR1-4) ATP competitive inhibitor that prevents downstream phosphorylation and activation of FGFR targets. Notably, FGFR3 alterations in urothelial carcinoma are prevalent, specifically in low-grade Ta disease.
Dr. Iyer then discussed THOR cohort 1, a phase 3 trial assessing erdafitinib versus chemotherapy in patients with metastatic urothelial carcinoma.1 Patients ≥18 years of age with unresectable advanced/metastatic urothelial cancer and select FGFR3/2alt (mutations/fusions), ECOG performance status 0-2, adequate organ function, progression on/after prior systemic therapy that included an anti-PD-(L)1 agent, and ≤2 prior lines of therapy were randomized 1:1 to receive erdafitinib (8 mg with pharmacodynamically guided up-titration to 9 mg on day 14) QD or investigator’s choice of chemotherapy (docetaxel or vinflunine) Q3W until disease progression or intolerable toxicity. The primary endpoint was overall survival, and secondary end points included progression-free survival, objective response rate, and safety. The trial design for cohort 1 is as follows: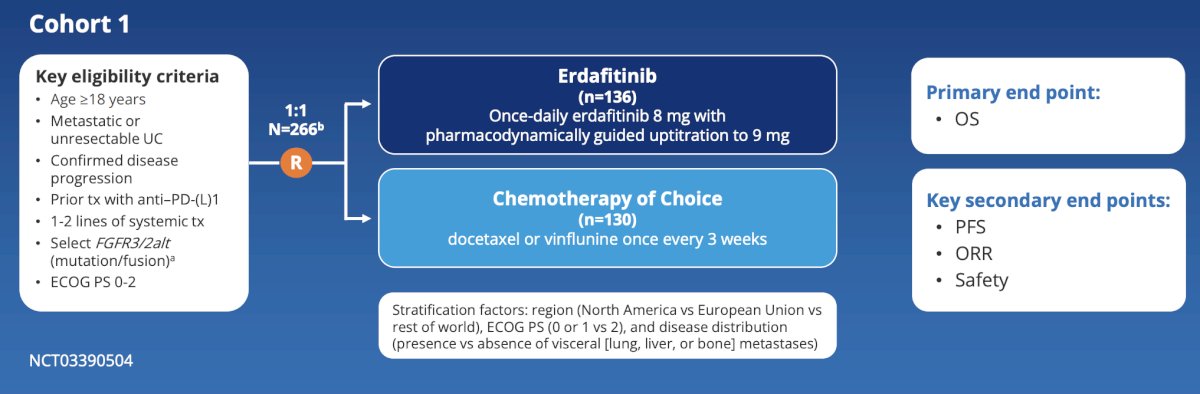
The median follow-up was 15.9 months over which the primary endpoint of the study was met, with erdafitinib significantly increasing overall survival and reducing the risk of death versus chemotherapy: median overall survival 12.1 months vs 7.8 months, HR 0.64, 95% CI 0.47-0.88: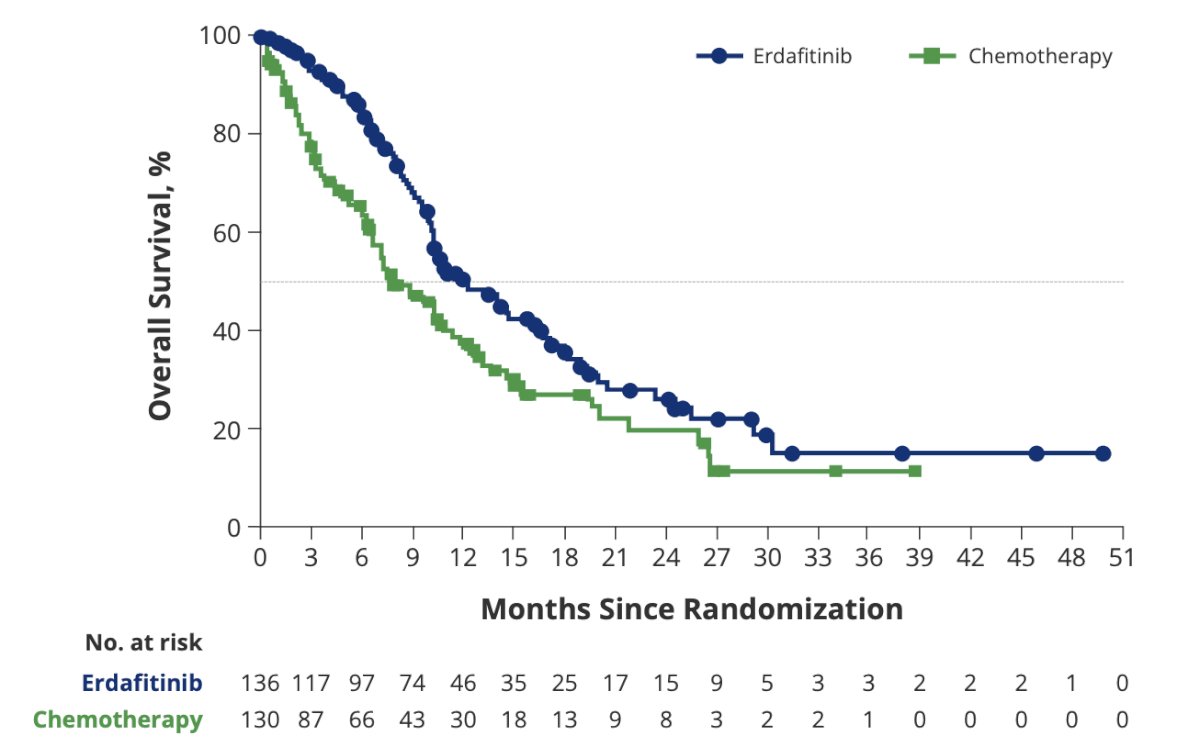
Furthermore, objective response rate was significantly higher for erdafitinib vs chemotherapy (45.6% vs 11.5%; relative risk 3.94, 95% CI 2.37-6.57, p < 0.001):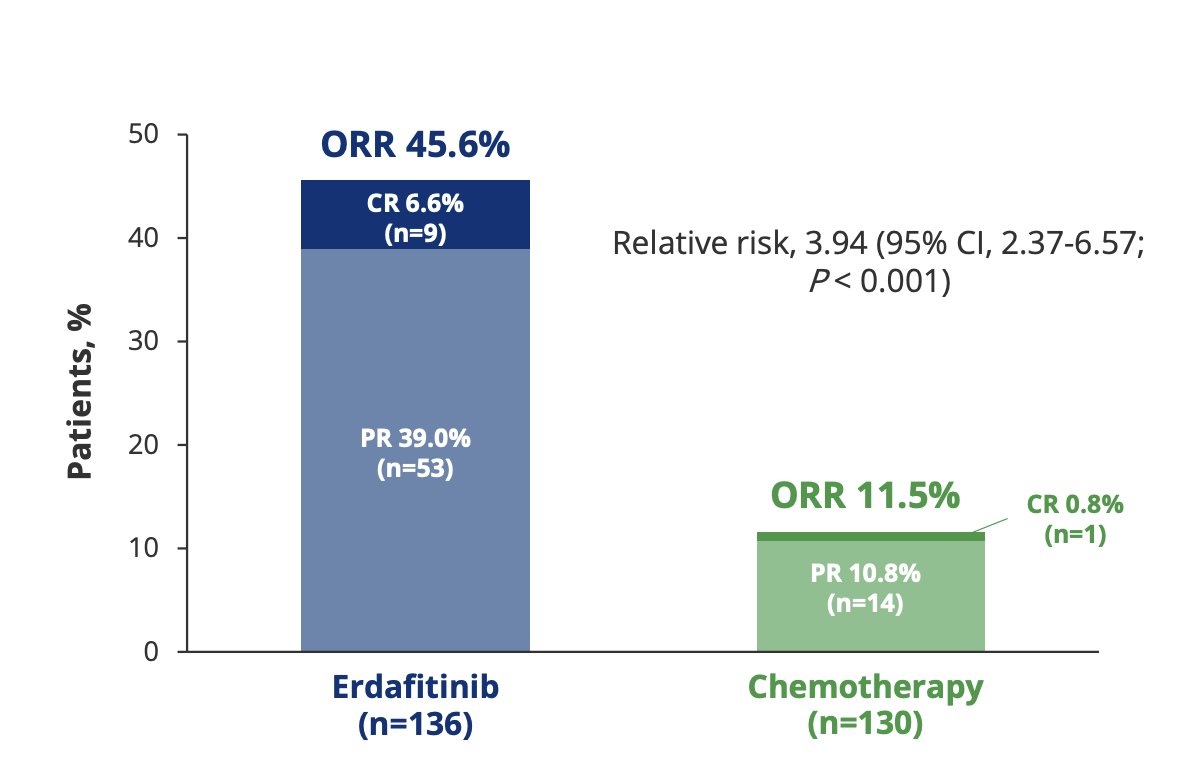
Based on these results, erdafitinib received FDA approval for patients with locally advanced or metastatic urothelial carcinoma with susceptible FGFR3 gene alterations whose disease has progressed on or after at least one line of prior systemic therapy. However, toxicity with oral erdafitinib is an issue. In THOR cohort 1, the safety profiles were consistent with the known profiles of erdafitinib and chemotherapy. Serious treatment-related adverse events were observed in 13.3% and 24.1% of patients with erdafitinib and chemotherapy, respectively, and grade 3/4 treatment-related adverse events were observed in 45.9% and 46.4% of patients with erdafitinib and chemotherapy, respectively: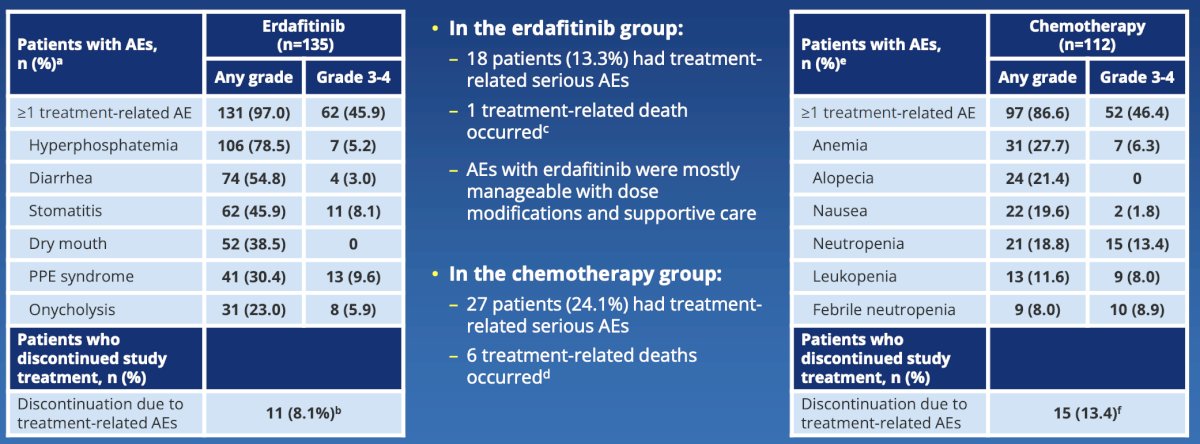
THOR-2 assessed erdafitinib for recurrent BCG-treated high-risk NMIBC, with the rationale being that although radical cystectomy is the standard of care for recurrent high risk NMIBC after intravesical BCG therapy, additional agents are needed. To date, there are several approved options, including intravesical chemotherapy, pembrolizumab, nadofaragene firadenovec, and N-803 + BCG. Because 1/3 of patients with high risk papillary NMIBC harbor FGFR3/2 alterations, can erdafitinib be leveraged in a post-BCG population as an alternative to radical cystectomy? The trial design for THOR-2 Cohort 1 is as follows:2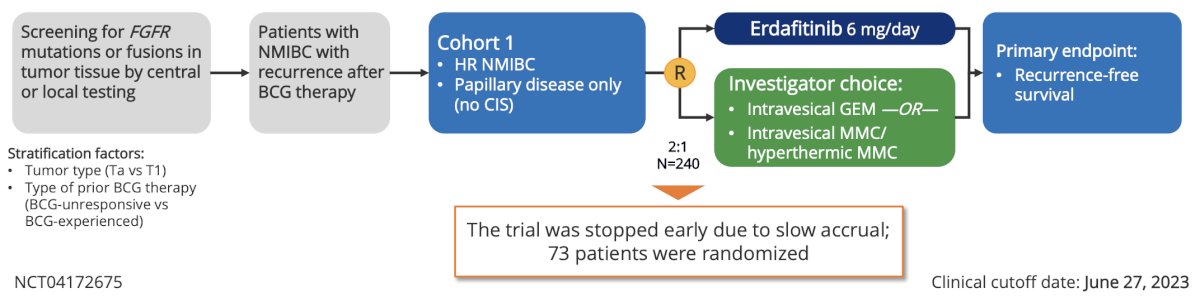
Overall there were 73 of the planned 240 patients randomized, but the study was stopped due to poor accrual, with the reasons being multifactorial: COVID-19, inadequate tissue for testing, BCG shortages, and systemic toxicity concerns. Among 49 patients who received at least 1 dose of erdafitinib, 28 discontinued study treatment, of which 50% were secondary to adverse events. However, the median follow-up was 13.4 months for both groups, and median recurrence-free survival was not reached for erdafitinib and was 11.6 months for chemotherapy, with an estimated hazard ratio of 0.28 (95% CI 0.10-0.60):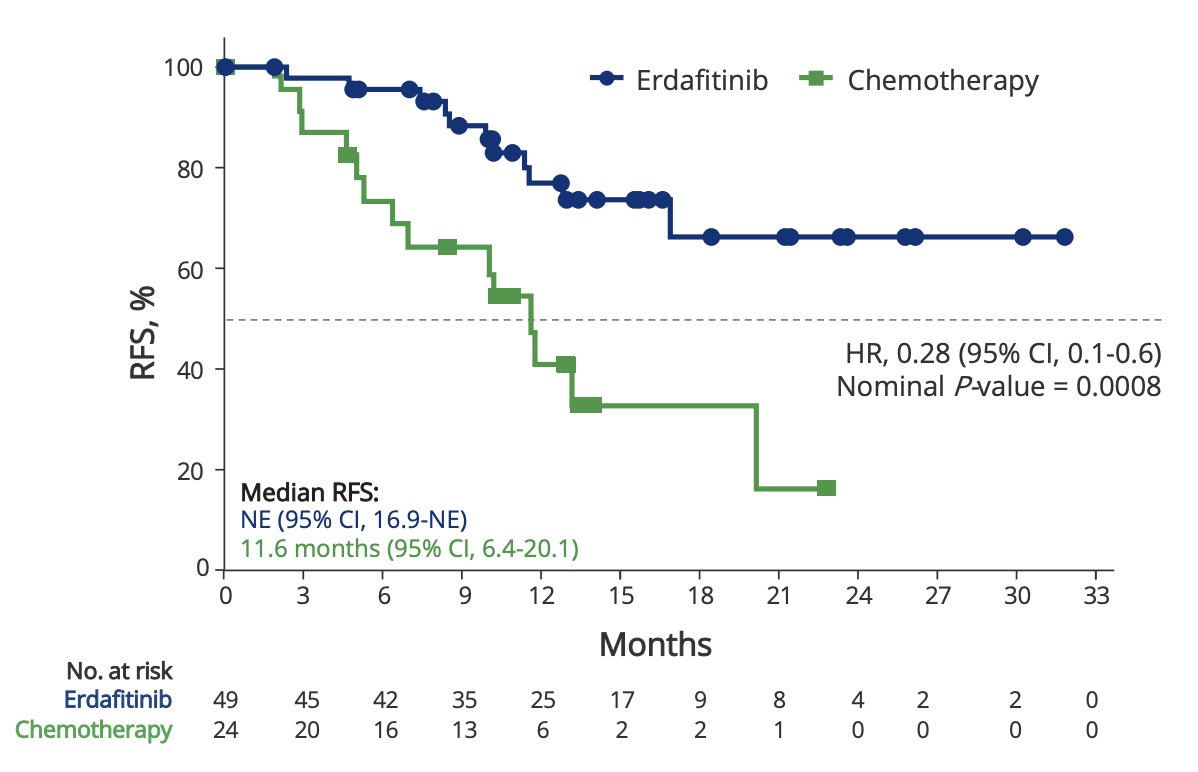
The 6- and 12-month recurrence-free survival rates were 96% and 77% for erdafitinib, compared to 73% and 41% for chemotherapy, respectively. Additionally, erdafitinib demonstrated a consistent recurrence-free survival benefit across subgroups, specifically tumor stage and prior BCG (experienced versus unresponsive):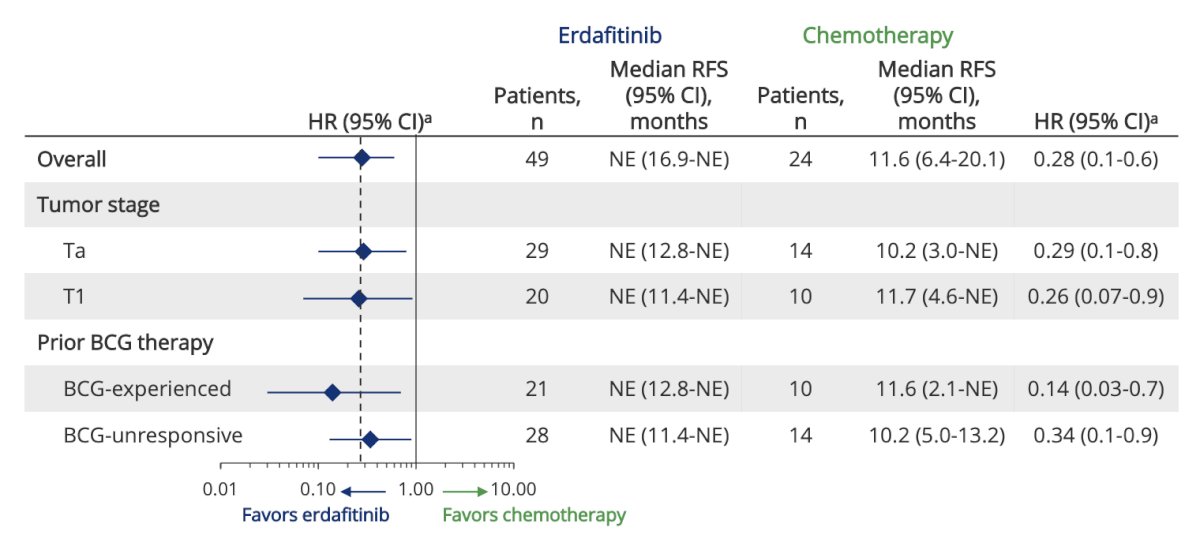
THOR-2 Cohort 2 is an exploratory cohort of patients with BCG-unresponsive CIS who harbor FGFR alterations, with or without papillary disease. The study design is summarized below: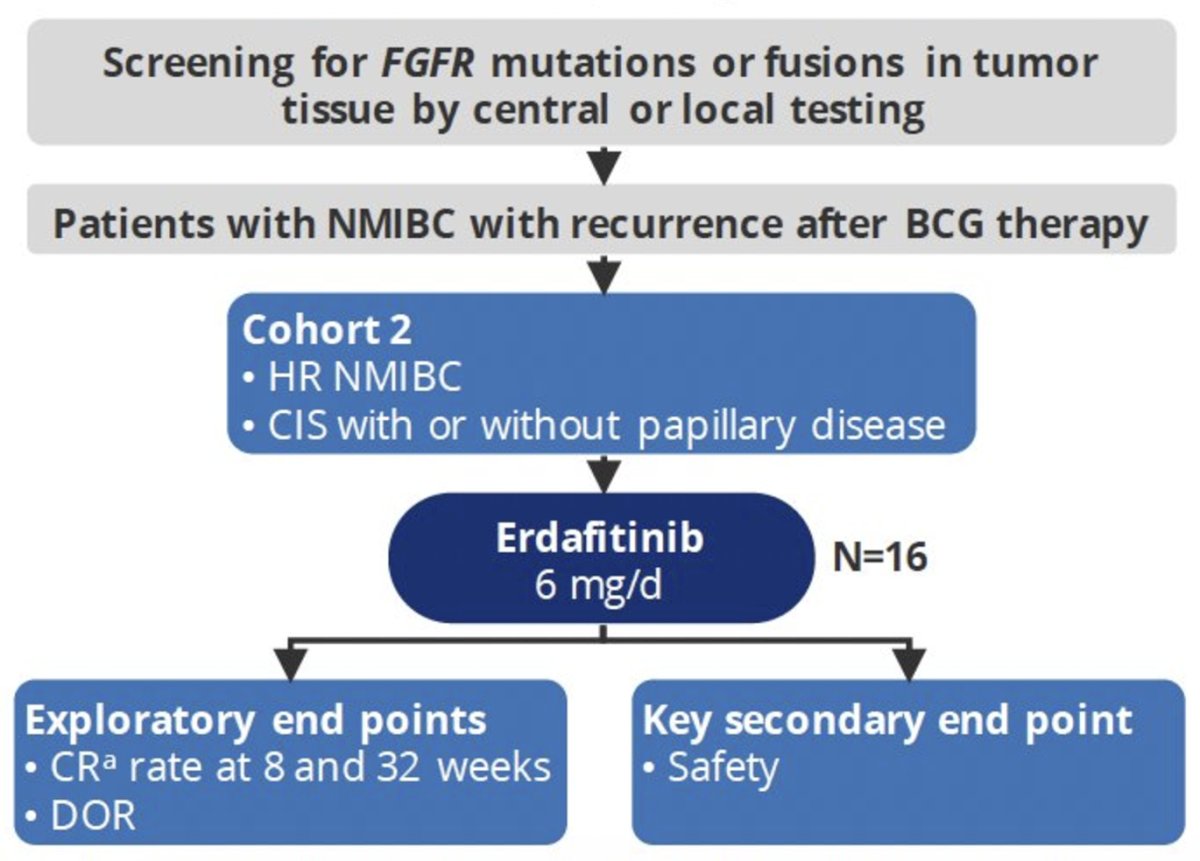
From an efficacy standpoint, the complete response rate in disease-evaluable patients was 94% (15/16) at 8 weeks and 73% (8/11) at 32 weeks. The median duration of response was not reached; 12 patient responses were ongoing at data cut-off.
THOR-2 Cohort 3 is an exploratory marker lesion cohort of patients with low-grade, intermediate-risk NMIBC. The study design is as follows: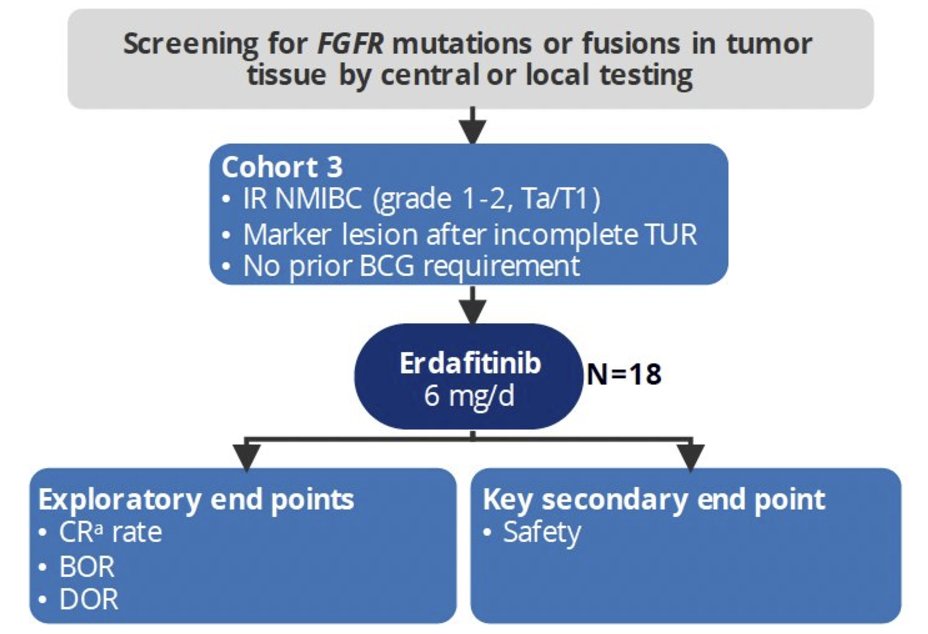
Overall, 15/18 (83%) patients had a complete response, two (11%) had a partial response, and one (5.6%) had high-grade recurrence as the best objective response. The median time to response was 1.15 months. Among the 17 responders, the median duration of response was 12.7 months, with 12 patient responses ongoing, three censored, and two ending with recurrence (1 low grade and high grade each) at the data cut-off.
Dr. Iyer then discussed TAR-210, which allows intravesical delivery of erdafitinib. The drug delivery device (the “pretzel”) is inserted through a catheter, which allows local, continuous release of erdafitinib over 90 days, reducing systemic toxicities of erdafitinib in patients with early stage disease. The device is then exchanged every 3 months. The first results of a phase 1 study assessing safety and efficacy were presented at EAU 2024 by Dr. Antoni Vilaseca. Cohort 1 patients had recurrent, BCG-experienced high-risk non–muscle-invasive bladder cancer (high-grade Ta/T1; papillary only) and refused or were ineligible for radical cystectomy. Cohort 3 patients had recurrent, intermediate-risk non–muscle-invasive bladder cancer (Ta/T1) with a history of only low-grade papillary disease. Before treatment, Cohort 1 patients must have all visible disease resected, whereas Cohort 3 required the presence of visible tumors. TAR-210 systems with two different erdafitinib release rates were evaluated. Response was assessed every 3 months with continued treatment for up to 1 year if recurrence-free (Cohort 1) or in complete response (Cohort 3). The trial design is as follows:
As of August 29, 2023, 16 patients in Cohort 1 and 27 patients in Cohort 3 have been treated with all tumors in both cohorts being recurrent. The Table 1 baseline characteristics are as follows: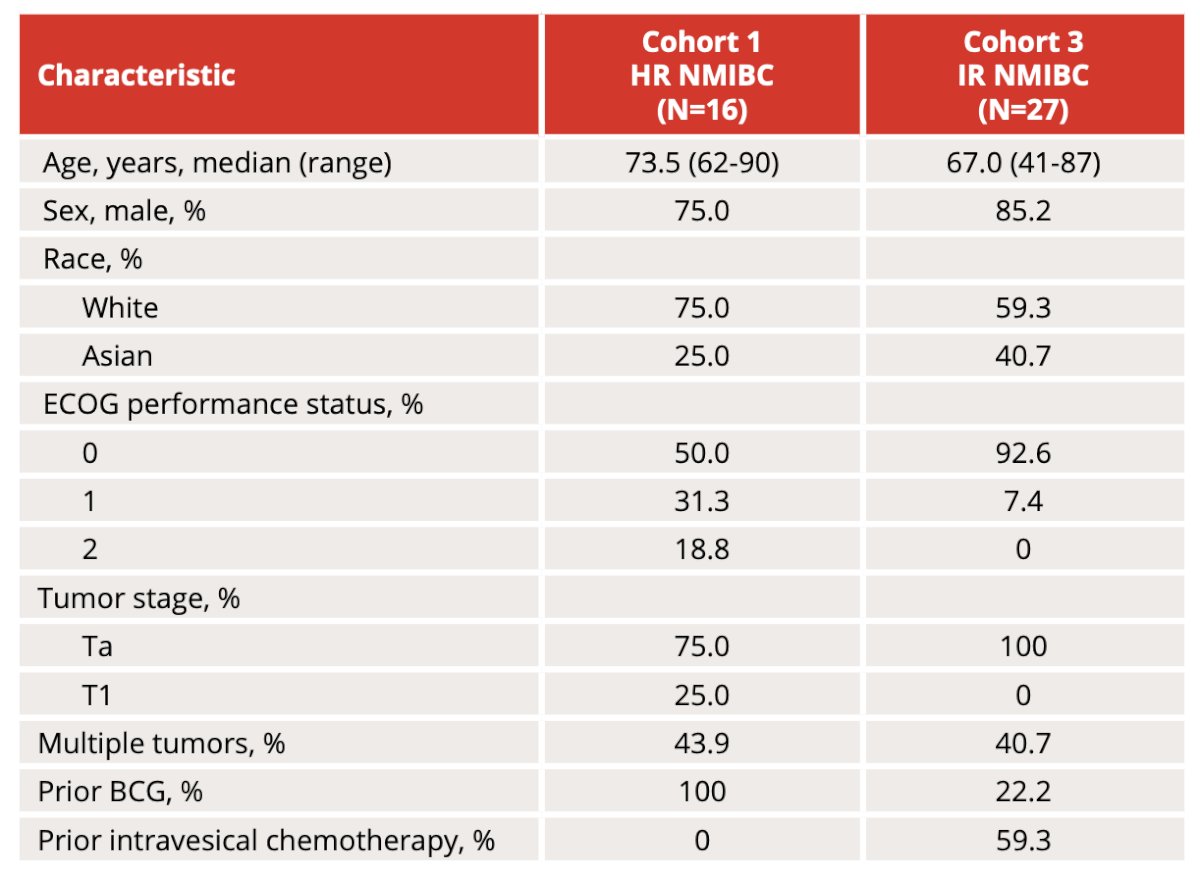
In cohort 1, 11 patients had response assessment and 9 were recurrence-free (recurrence-free rate of 82%):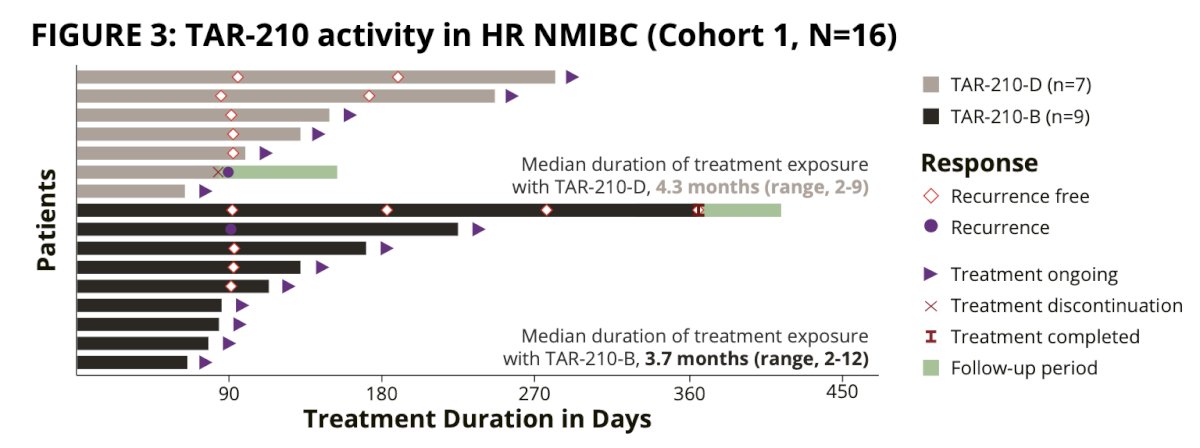
Median recurrence-free survival in Cohort 1 was non-estimable 95% CI 2.96 months to nonestimable. In cohort 3, 15 patients had a response assessment and 13 achieved a complete response (rate: 87%):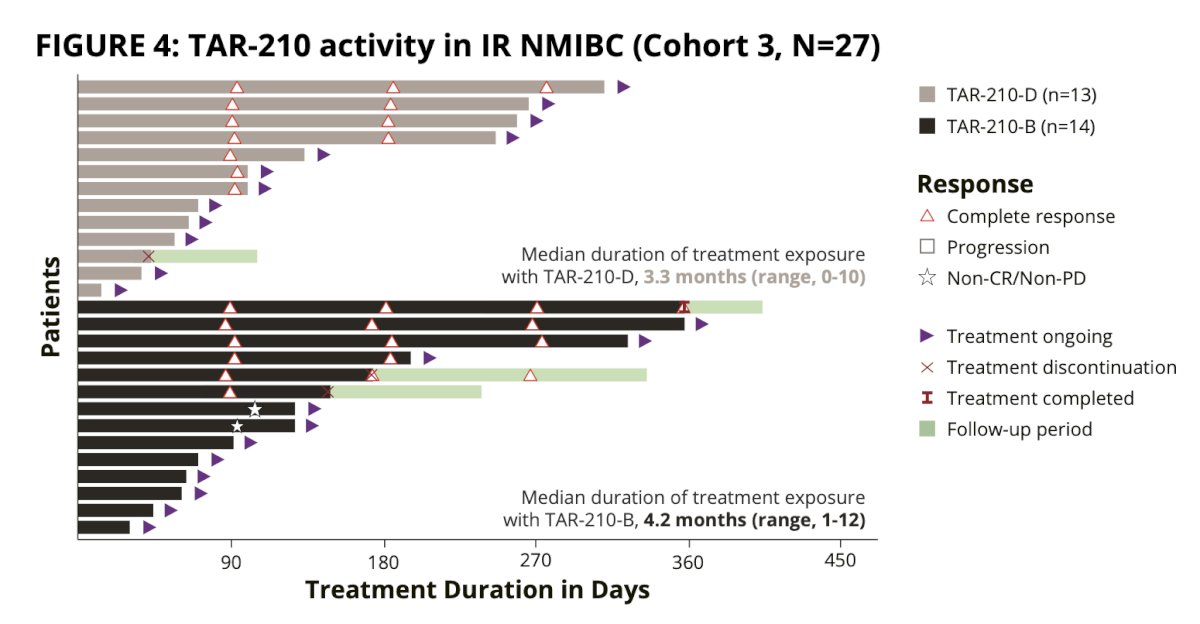
The most common treatment-related adverse events were grade 1/2 lower urinary tract adverse events. There were no dose-limiting toxicities. Two patients discontinued treatment due to adverse events of low-grade urinary symptoms, and one patient had serious adverse events of pyelonephritis and sepsis (unrelated to TAR-210). No deaths were reported: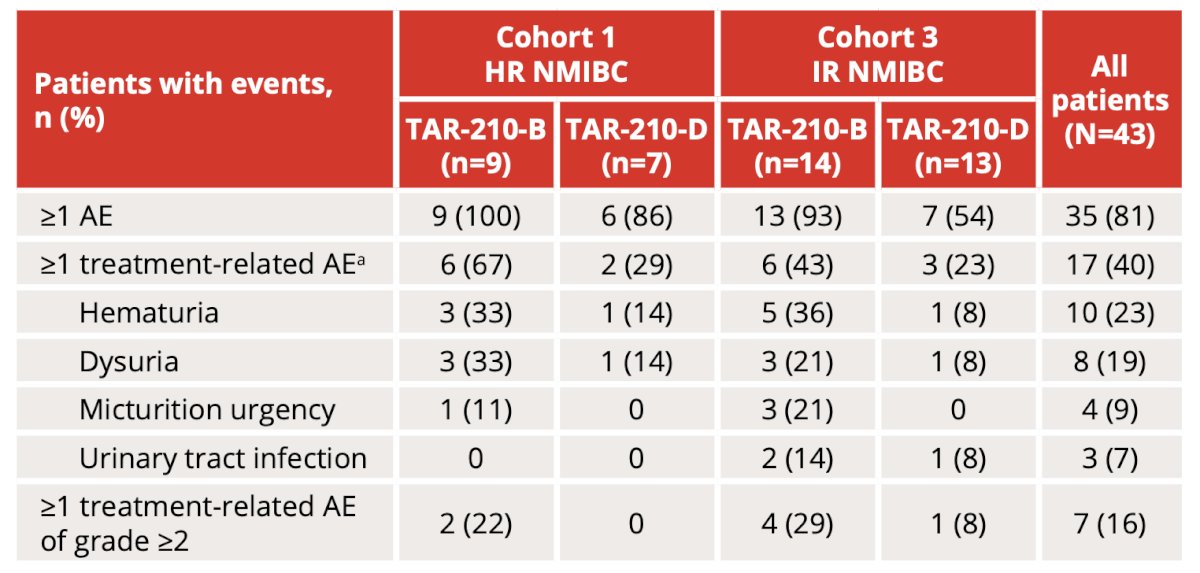
The aforementioned data led to MoonRISe-1, a phase 3 trial assessing intermediate risk non-muscle invasive bladder cancer, as well as FGFR2/3 alterations by central or local tissue or urine testing. Patients (n = 540) are being randomized 1:1 to TAR-210 versus investigator’s choice of intravesical chemotherapy (mitomycin C or gemcitabine). The primary endpoint is disease-free survival and the trial design for MoonRISe-1 is as follows: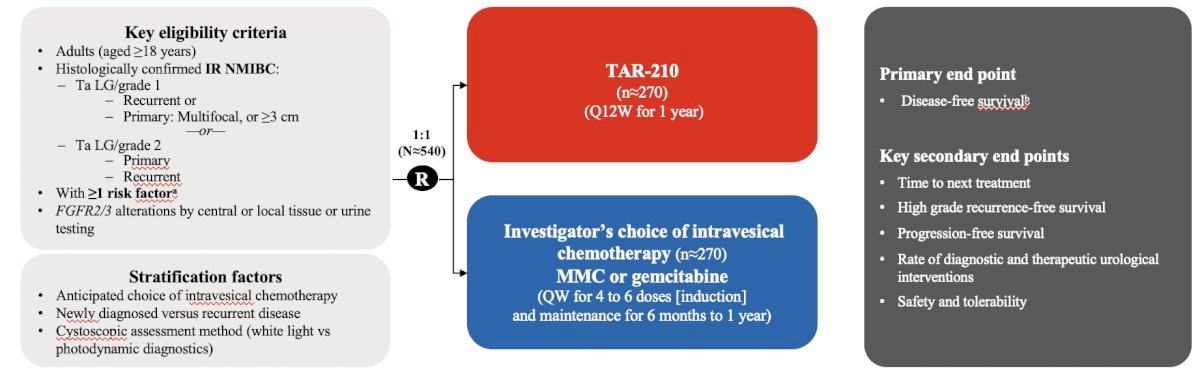
In the muscle invasive bladder cancer disease space, the SOGUG-NEOWIN phase 2 trial is assessing neoadjuvant erdafitinib +/- cetrelimab in cisplatin-ineligible patients. Eligible patients are those with cT2-4aN0-1M0 urothelial carcinoma who test positive for FGFR mutations and are ineligible for or refuse neoadjuvant cisplatin. Ninety patients will be randomized to daily erdafitinib monotherapy versus combination erdafitinib + cetrelimab. The co-primary study endpoints are pathologic complete response and downstaging (i.e., <ypT2) rates. The trial design is as follows: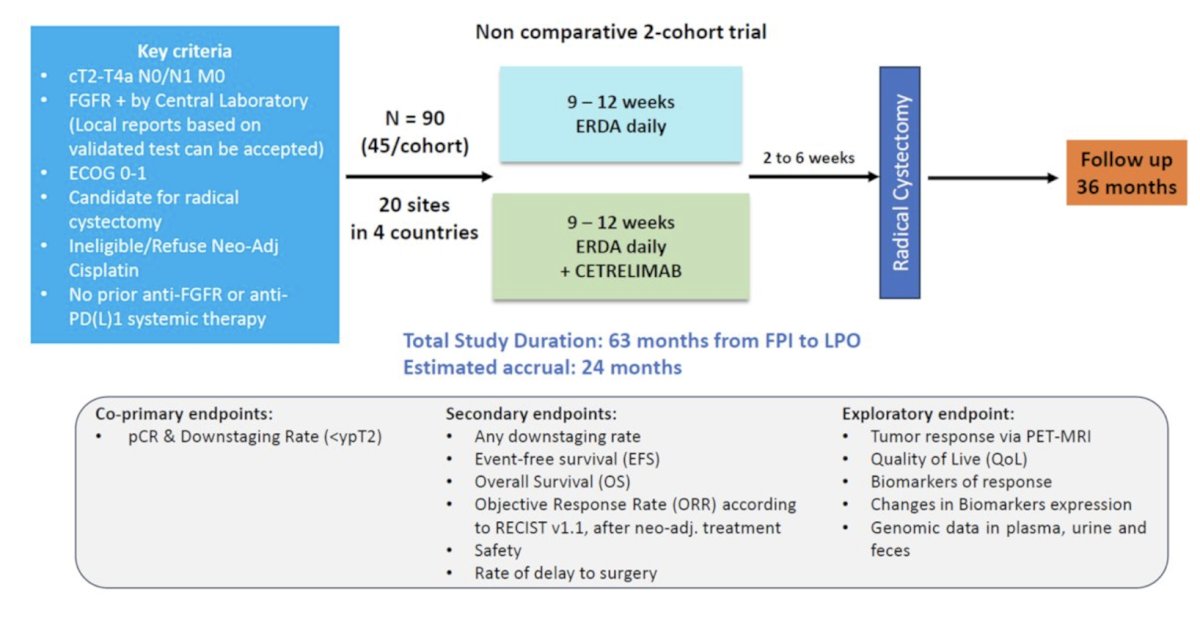
Dr. Iyer concluded his presentation discussing FGFR and precision in urothelial carcinoma with the following take home messages:
- FGFR3 actionable alterations are detected across stages of urothelial carcinoma
- Erdafitinib is the only targeted therapy FDA-approved for patients with FGFR3-altered locally advanced or metastatic urothelial carcinoma that has progressed after at least one line of systemic therapy based on an overall survival benefit compared to second-line single agent chemotherapy.
- Erdafitinib is actively being explored in patients with muscle invasive bladder cancer and NMIBC
- Oral therapy is active but limited by systemic toxicity
- TAR-210 represents an intravesical formulation of erdafitinib with limited systemic toxicity and early evidence of significant efficacy in NMIBC
Presented by: Gopa Iyer, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 Society of Urologic Oncology (SUO) Annual Meeting, Dallas, TX, Tues, Dec 3 – Fri, Dec 6, 2024.
References: