(UroToday.com) The 2022 WCET Annual meeting featured a session titled “clinical stones” highlighting multiple studies from Dr. Clayman and colleagues at the University of California, Irvine (UCI). The featured on-going study sought to explore the maximum ureteral circumference that can be attained safely using the teams novel force-reading sensor. The team at UCI looked at several pre-operative factors that could potentially influence the ability of the ureter to dilate to its respective maximum size. Dilating the ureter and allowing the passage of a larger Ureteral Access Sheath leads to increased surgical efficiency at no cost of injury.1
The sample size of each group in this study is small, however, statistical analysis has found significant association of what might influence ureter diameter. Results from this study bring routine pre-operative treatment into the spotlight, but a larger sample size is needed to declare different correlations.
The study has so far recruited 54 patients (24 male, 30 female) with CT-confirmed renal stones undergoing a ureteroscopy or percutaneous nephrolithotomy procedure. During the surgical procedure, 37-centimeter Cook® urethral dilators were inserted into the ureter concertedly with the UCI Force Sensor. Dilators started at 10 French (Fr) and increased by 2 Fr until a force of 6 Newtons (N) was reached when inserting in a dilator. 6 N is the safety threshold that was clinically determined when passing Ureteral Access Sheaths (UAS) in earlier porcine and human UCI studies.2,3 A UAS size was then chosen based on the largest successful dilator passed, a max UAS size of 16 Fr. Following the procedure, a ureteroscopic inspection was performed to determine if any ureteral injury occurred, this was determined using the post-ureteroscopic lesion scale (PULS) which ranges from 0-5, a grade of 3 and above is defined as a significant injury.
In all ureters examined that stayed at or below the 6 N threshold, 67% accepted at least a 14 Fr dilator with no ureteral injury, while 43% accepted at least a 16 Fr dilator where 1 PULS grade of 3 was recorded. 18% of ureters allowed a safe passage of an 18 Fr dilator or more, the maximum size being 24 Fr, while only recording one PULS 3 Grade. The 54 patients were then analyzed depending on the pre-operative treatment they received, a total of 4 separate groups (Figure 2). Patients with an indwelling stent prior to their surgery was associated with the ability to pass a larger dilator size compared to those without stents (Figure 2A; 17.3 Fr vs 13.9 Fr; p = 0.004). Interestingly, the use of tamsulosin was not associated with being able to pass larger dilator sizes compared to patients who received no pretreatment (Figure 2A; 13.76 vs 14.25; p = 0.2985, 95% CI [-2.354, 1.3834]).
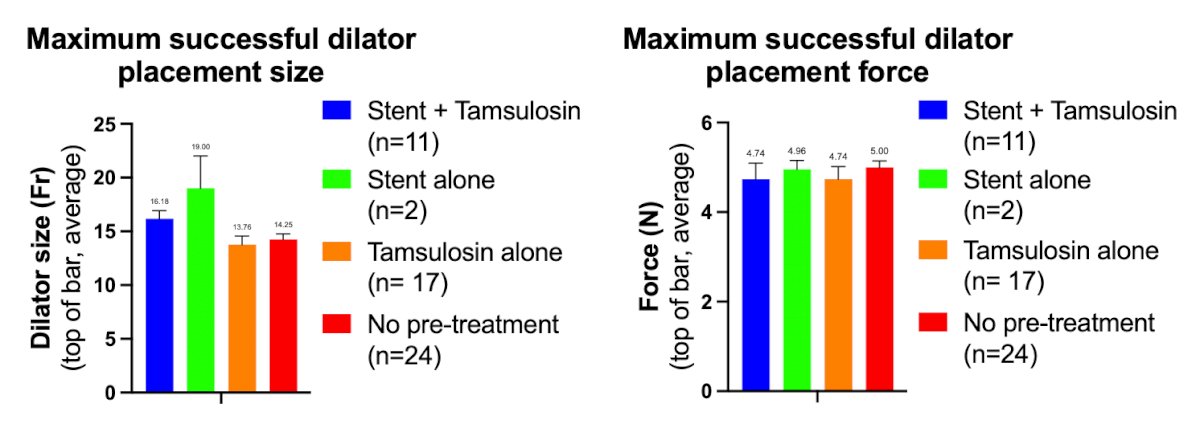
Figure 2. (A) The average dilator placement size for each of the 4 treatment groups was greater than 14 Fr and (B) the average maximum force for all groups during successful dilation was 5 N.
The UCI team have concluded that at forces less than or equal to 6N, 67% of ureters accommodated a 14 Fr dilator, almost half of ureters (43%) dilate up to 16 Fr and patients with indwelling stents saw a 3.4 Fr larger dilator passed compared to those without stents. The conclusions have indications of how a urologist might treat a patient before and during a stone extraction surgery. Although too early to tell, results from this study give slight indications that prescribing tamsulosin, a common practice, does not help facilitate a safe passing of a larger sheath. While sample size of the study is relatively small, the results of a larger study can have an impact on how urologist pre-operatively treat their patients in hopes of dilating the ureter to its respective maximum size.
Presented by: Paul Piedras, BS, University of California Irvine
Written by: Paul Piedras, BS, University of California Irvine, @piedras_paul on Twitter during the 39th World Congress of Endo urology and Uro-Technology (WCET), Oct 1 - 4, 2022, San Diego, California.
References:
- Tracy CR, Ghareeb GM, Paul CJ, Brooks NA. Increasing the size of ureteral access sheath during retrograde intrarenal surgery improves surgical efficiency without increasing complications. World J Urol. 2018 Jun;36(6):971-978. doi: 10.1007/s00345-018-2204-z. Epub 2018 Jan 27. PMID: 29380131
- Kaler KS, Lama DJ, Safiullah S, Cooper V, Valley ZA, O'Leary ML, Patel RM, Klopfer MJ, Li GP, Landman J, Clayman RV. Ureteral Access Sheath Deployment: How Much Force Is Too Much? Initial Studies with a Novel Ureteral Access Sheath Force Sensor in the Porcine Ureter. J Endourol. 2019 Sep;33(9):712-718. doi: 10.1089/end.2019.0211. Epub 2019 Jul 2. PMID: 31161788.
- Tapiero S, Kaler KS, Jiang P, Lu S, Cottone C, Patel RM, Okhunov Z, Klopfer MJ, Landman J, Clayman RV. Determining the Safety Threshold for the Passage of a Ureteral Access Sheath in Clinical Practice Using a Purpose-Built Force Sensor. J Urol. 2021 Aug;206(2):364-372. doi: 10.1097/JU.0000000000001719. Epub 2021 Mar 29. PMID: 33780267.