Approximately 6000 robotic cases have been performed in Dr. Hemal’s center. Almost 50% of them were robotic prostatectomy, 11% nephrectomy, 20% partial nephrectomy, 7% pyeloplasty, 5% radical cystectomy, and the rest included other procedures.
In the S/Si – the robot can be docked perpendicular to the operation table. In contrast, the Xi is optimized for multi-quadrant surgery. A great advantage of the Xi robot is the feature of camera port hopping. If moving from proximal to distal, the camera may be moved one port caudally, and the robotic instruments can be exchanged as desired without undocking. The retargeting feature may also be utilized to improve triangulation and ergonomics. This saves a significant amount of time and increases versatility.
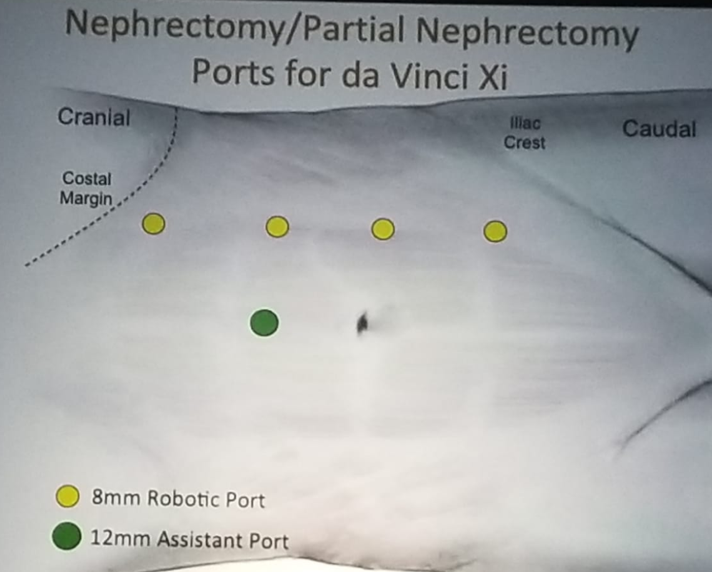
The suggested port placement for nephrectomy and partial nephrectomy for the Si/S and Xi systems are shown in figure 1 and figure 2, respectively. Also, the recommended port placement for retroperitoneal robotic partial nephrectomy is shown in figure 3. As for robotic nephroureterectomy, port placement should be done in the Si and Xi, as shown in figure 4, and 5, respectively.
Figure 1:

Figure 2:

Figure 3: Port placement for retroperitoneal robotic partial nephrectomy:
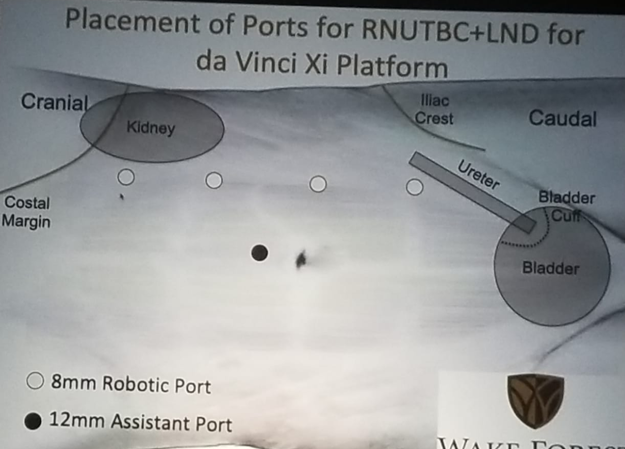
Figure 4:

Figure 5:

Dr. Hemal moved on to discuss the various techniques for robotic radical prostatectomy. These include the transperitoneal standard approach (antegrade vs. retrograde), posterior approach, extraperitoneal, Retzius sparing, perineal prostatectomy, perineal single incision, and an abdominal single port. The port placement recommendation for the transperitoneal standard approach is shown in figure 6 and 7, for the Si and Xi, respectively. Lastly, Dr. Hemal presented the recommendation of port placement when performing a robotic retroperitoneal lymph node dissection (Figure 8).
Figure 6:

Figure 7:
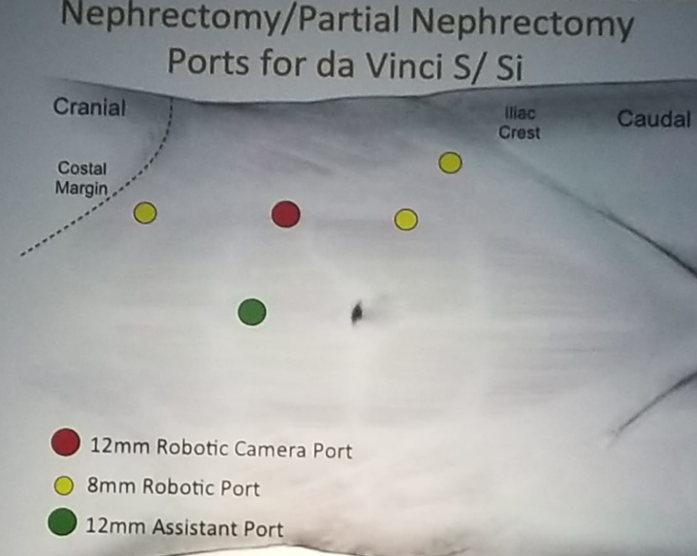
Figure 8:
Dr. Hamel concluded his overview, emphasizing that patient biology, size, and location of the target organ are critical in consideration of port placement in robotic surgery. We also need to consider the patient’s body habitus and the history of previous operations. The surgeon must be versatile and acquire knowledge on as many different techniques as he can, as different techniques are needed in different situations. Finally, the surgeon should always insert the camera port first, to delineate the exact anatomy of the patient.
Presented by: Ashok Hemal, MD, Wake Forest School of Medicine, Winston-Salem, North Carolina, United States
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at 2019 3rd Annual North American Robotic Urology Symposium (NARUS), February 8-9, 2018 - Las Vegas, Nevada, United States