Before performing a robotic partial nephrectomy, the surgeon must conduct a thorough preoperative assessment of the patient’s anatomy, and especially the renal and surrounding vessels. Axial imaging should be used (CT/MRI), and 3D reconstruction of the relevant vasculature is most helpful. The usage of intraoperative ultrasound is recommended and has been shown to help surgeons understand tumor anatomy. Following the preoperative assessment, an operative strategy should be formulated, and contingency plans for various scenarios should be made as well.
Hilar control is one of the most important steps in robotic partial nephrectomy. All arteries and veins must be isolated and skeletonized appropriately. If the tumor is large and central, the vein must be controlled as well. Lastly, the bulldogs must be placed carefully, either by the surgeon or the assistant, and the Scanlan® are the preferred choice. There are various clamping options, and it is important for the surgeon to recognize and be familiar with the various options (Figure 1).
Figure 1 – Various Available Clamp Options:
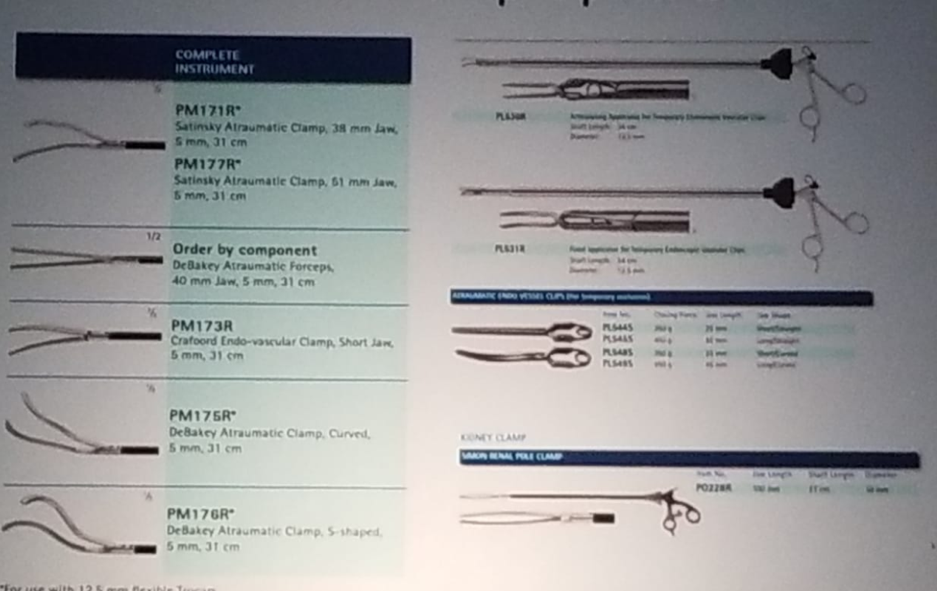
If the tumor is deep, the skeletonization of the vessels is most important, especially of the arteries, as periarterial tissue can prevent occlusion via the clamp. If the plan is not to clamp the vein, it should be prepared just in case, with the usage of vessel loops on all hilar vessels, so that they could be found quickly if needed. The bulldogs should be applied with a 2-3 mm separation, and it is important to make sure that the bulldog end tip is applied to the artery, as it holds maximum compression at its tip. It is also advisable to use Indocyanine green (ICG) through the da Vinci® Firefly fluorescence imaging system, to check for ischemia. ICG is used as a marker in the assessment of the perfusion of tissues and organs. The light needed for the excitation of the fluorescence is generated by a near-infrared light source which is attached directly to the robotic camera. The ICG can be used for better identification of renal vasculature, confirmation of hilar ischemia (complete vs. segmental), and for tumor margin identification.
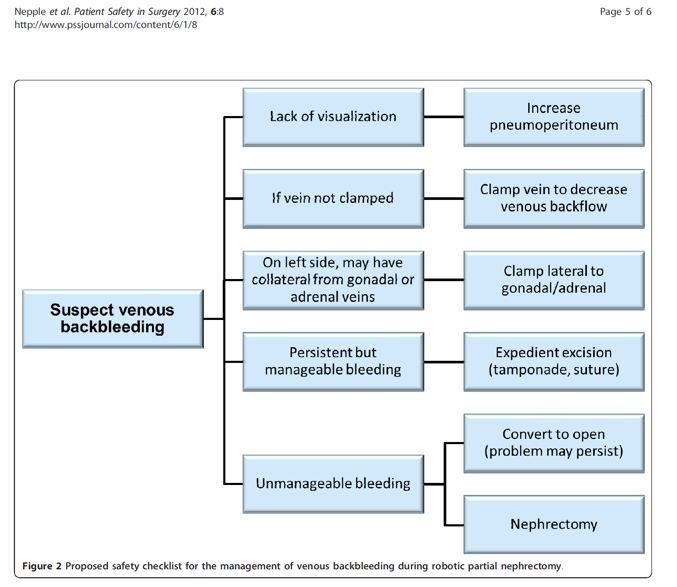
Dr. Herrel mentioned an important paper, describing a multicenter safety checklist for intraoperative hemorrhage control while clamped during robotic partial nephrectomy.1 This paper demonstrates a constructive algorithm showing the actions that are required when there is evidence for arterial and venous bleeding (Figure 2 and 3).
Figure 2 – Algorithm for Suspected Arterial Bleeding During Clamped Robotic Partial Nephrectomy
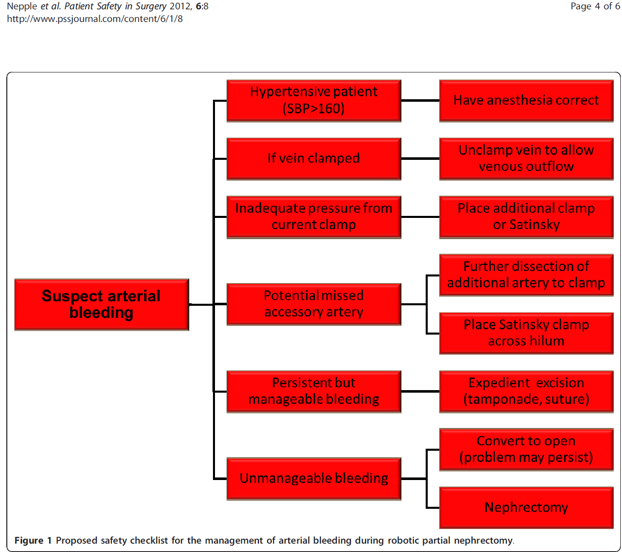
Figure 3 – Algorithm for Suspected Venous Bleeding During Clamped Robotic Partial Nephrectomy
Lastly, when severe bleeding occurs, it is important to follow several simple steps. First, the surgeon must remain calm, and take some deep breaths. At this stage, it is important to acquire another circulator nurse in the room, ready the “open” trays for possible conversion, and call another colleague for assistance.
Presented by: S. Duke Herrell, MD, Professor of Urologic Surgery, Professor of Biomedical Engineering
Vanderbilt University Medical Center
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at 2019 3rd Annual North American Robotic Urology Symposium (NARUS), February 8-9, 2018 - Las Vegas, Nevada, United States
References:
1. Nepple KG et al. Patient Safety in Surgery 2012
Further Related Content:
Kidney Hilum – Full Clamp