The rate of genitourinary injury during gynecologic procedures is 0.3% in benign gynecological laparoscopy, with electrocautery being the most common cause. These injuries are more common with lap assisted vaginal hysterectomy, endometriosis, and prior surgery. Lower rates of ureteral injury are associated with supracervical hysterectomy. Bladder injury is three times more common than ureteral injury.
When approaching such a patient with a ureteral injury, there should be a clear evaluation framework. This includes patient factors – whether there is family available, is the patient hemodynamically stable, knowledge of the relevant patient comorbidities (urologic, gastrointestinal, previous radiotherapy, malnutrition, and previous chemotherapy), and whether the patient has a normal contralateral kidney. Furthermore, the hospital setting needs to be taken into account – is the patient in the OR, and whether there is available urologic staff that knows how to work with the robot. Lastly, the surgical treatment strategy needs to be understood from the beginning – anesthesia should be involved, and the surgeon needs to decide on the positioning and approach of the procedure.
The immediate reconstructive options include ureteral reimplantation, ureteroureterostomy, psoas hitch, and Boari flap. Other less common options include appendix/ileal ureter, autotransplantation, and radical nephrectomy. In cases where there is a need for complex reconstruction, or there is uncertain pathology or prognosis, and in an unstable patient, it is preferable not to do the definitive surgery at that time, and to do what is minimally required, so that the patient could be definitively operated on another day. In these cases, it is advisable not to do nephrectomy, ureteroureterostomy, or attempt any complicated reconstructive procedures. It is preferable to bail out and return another day. The available treatment options for these situations include clipping of the ureter and placing a nephrostomy tube or a single J stent and bringing the ureter through the skin.
Over 50% of ureteral injuries are diagnosed postoperatively. Placing of stents may work for urine leaks but often heals with a stricture. A nephrostomy tube should be inserted when it is the goal to identify the stricture and give the ureter some “rest”. When planning surgical repair, it is best to go within five days of injury, or alternatively, to wait six weeks.
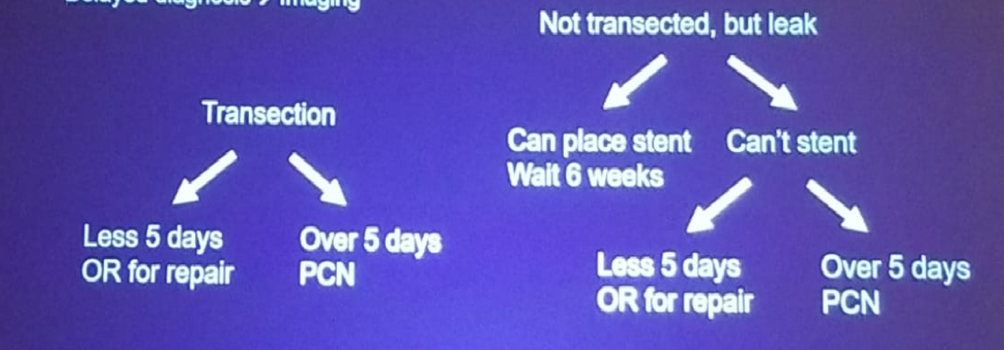
Dr. Zhao then concluded his talk and provided an algorithm of when and how to treat a ureteral injury caused intraoperatively (figure 1). Generally speaking, ureteral reimplantation should be attempted when there is an intraoperative ureteral injury in a favorable setting. If the setting is unfavorable, a nephrostomy tube should be inserted as soon as possible. When the diagnosis is delayed, it is important to rely on the most recent imaging and assess the magnitude of the injury.
Figure 1- Treatment Algorithm of the Ureteral Injury:
Lee Zhao, MD, board certified urologist, NYU Langone Health, New York, New York
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at 2019 3rd Annual North American Robotic Urology Symposium (NARUS), February 8-9, 2018 - Las Vegas, Nevada, United States