However, it is essential to focus on a decrease in bladder capacity as well for classical interstitial cystitis (Hunner’s ulcer type). The patients with this disease ultimately suffer from voiding dysfunction caused by lower compliance in the bladder and from reflux caused by severe fibrosis near the ulcer in the ureteral orifice area (Figures 1 & 2). Therefore, the preservation of bladder capacity is a critical problem along with the removal of ulcers in ulcerative interstitial cystitis patients.
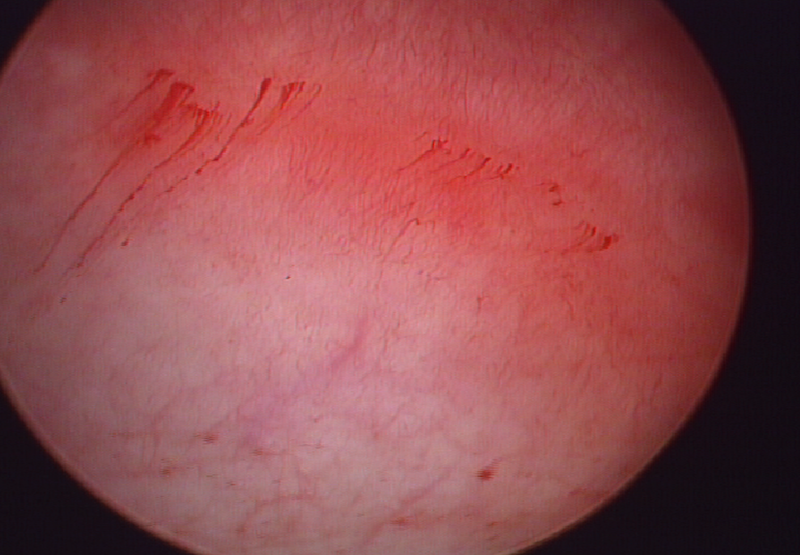
As ulcers persist longer, the fibrotic changes get severe near the tissue around ulcers. In Figure 3, It may seem that only an ulcer is present, but in Figure 4, a fibrotic bundle formation can be found on the ulcer base. Thus, the removal of an ulcer could improve pain, but the recovery of bladder capacity may not be expected.
Our treatment is similar to a treatment for urethral stricture that disconnects a fibrotic bundle through surgery. Therapeutic hydrodistention could disconnect the fibrotic bundle contracting the bladder that it may benefit the preservation of bladder capacity. As a result, transurethral resection (TUR) and therapeutic hydrodistention (combination procedure) in patients with ulcerative IC, 49.2% showed favorable outcomes for three years.
Traditionally, the hydrodistention procedure is widely used as a diagnostic tool for ulcer and non-ulcer types. However, excessive hydrodistention procedures may cause heavy bleeding which could prevent the complete removal of ulcers (Figure 5). Therefore, It is important to mark the pre-existing ulcers and to use the hydrodistention procedure to seek for hidden or unfound ulcers. When the patients were treated with complete transurethral resection of ulcer and followed by disconnection of a fibrotic bundle through therapeutic hydrodistention, the satisfaction of patients and the preservation of bladder capacity of patients improved.
Figure 1. 48-year-old woman with chronic pelvic pain, dysuria, and frequency. On cystoscopy, an area of normal bladder wall mucosa was seen between the Hunner lesion and left ureteral orifice (indicted by the arrow) seen adjacent to the Hunner lesion.
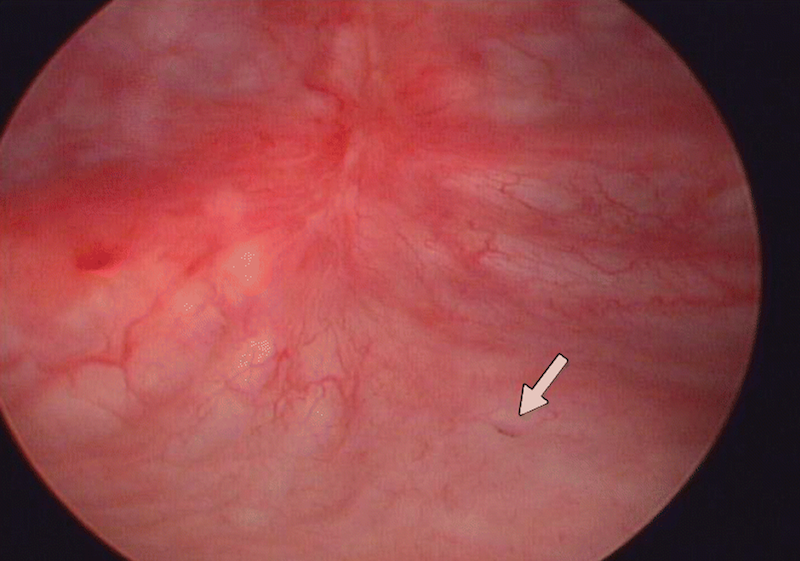
Figure 2. On voiding cystourethrography, a contrast agent (indicted by the arrow) refluxed into the non-dilated left ureter, but the renal pelvis was not visualized. There was no evidence of contrast agent reflux into the right ureter. Grade I left vesicoureteral reflux was confirmed.1
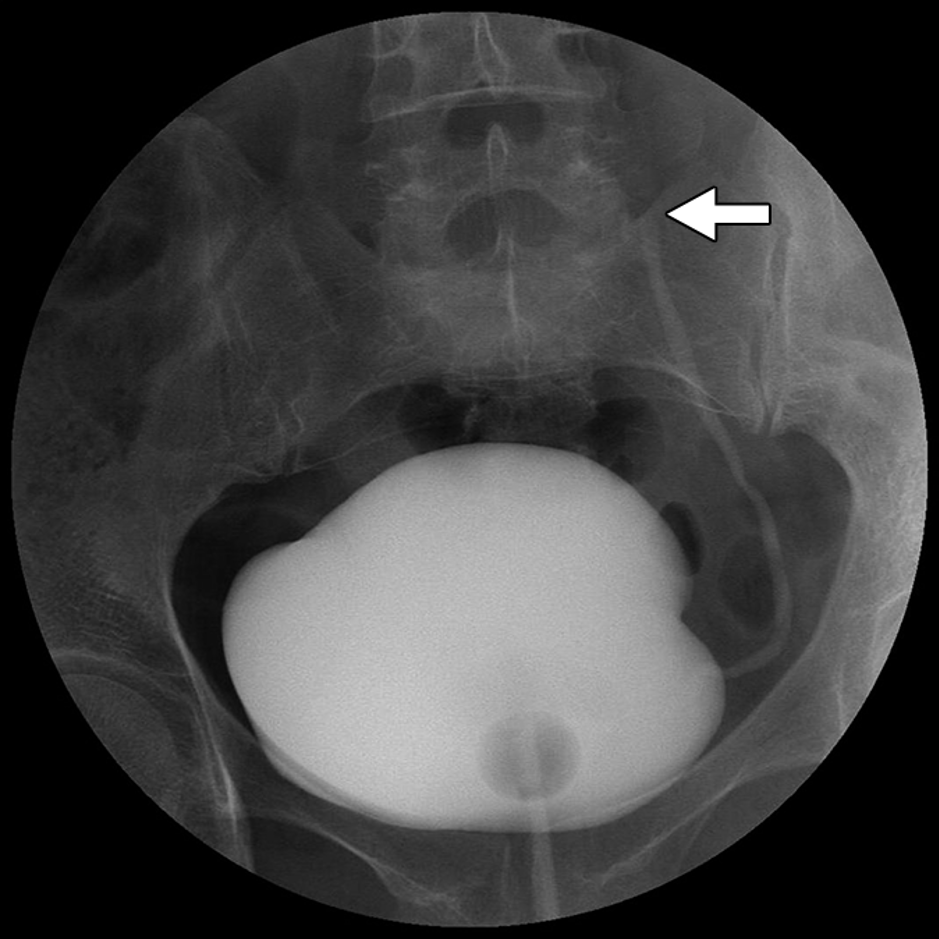
Figure 3. SIxty-five-year-old woman with ulcerative interstitial cystitis. On cystoscopy, an ulcer was observed before the bladder filling.

Figure 4. On cystoscopy, a fibrotic bundle was observed on the Hunner lesion as the bladder is filled.
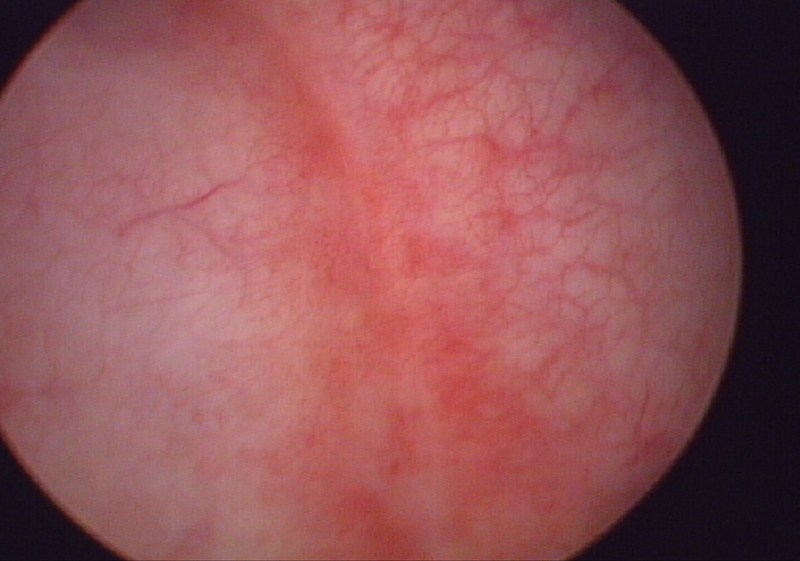
Figure 5. Diagnostic hydrodistention could cause bleeding which could prevent the complete removal of ulcers. Before diagnostic hydrodistention, the marking of pre-existing ulcers could benefit during the surgical procedure.
Written by: Young Ho Kim MD, PhD, Department of Urology, Soonchunhyang University Bucheon Hospital, Chief of Urology, The Soonchunhyang University of Korea, College of Medicine, Asan, South Korea
References:
- Lee, Ji Eun, Boem Ha Yi, Hae Kyung Lee, Min Hee Lee, and Young Ho Kim. "Correlation of cystoscopically confirmed periureterally located hunner lesion with vesicoureteral reflux: preliminary study in patients with interstitial cystitis." American Journal of Roentgenology 204, no. 4 (2015): W457-W460.
- Lee, Sang Wook, Woong Bin Kim, Kwang Woo Lee, Jun Mo Kim, Young Ho Kim, Bora Lee, and Jae Heon Kim. "Transurethral resection alone vs resection combined with therapeutic hydrodistention as treatment for ulcerative interstitial cystitis: initial experience with propensity score matching studies." Urology 99 (2017): 62-68.
- Whitmore, Kristene E., Magnus Fall, Atsushi Sengiku, Hikaru Tomoe, Yr Logadottir, and Young Ho Kim. "Hunner lesion versus non‐Hunner lesion interstitial cystitis/bladder pain syndrome." International Journal of Urology 26 (2019): 26-34.