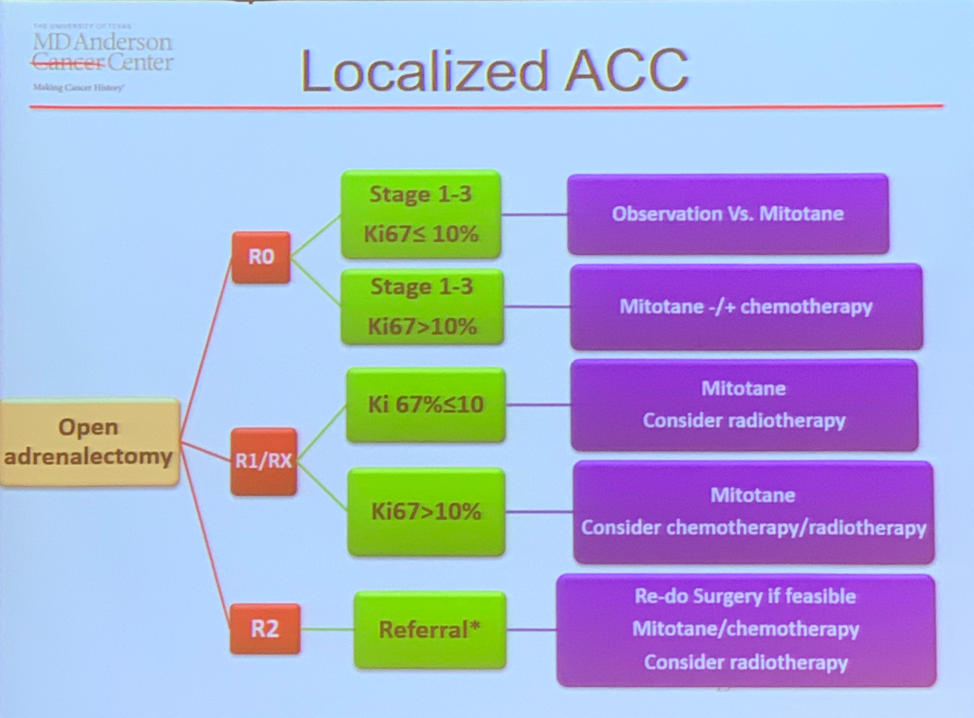
Metabolically active ACC has a worse overall survival than nonactive tumors related to the systemic effects of hormone oversecretion, such as hypertension, poor-glucose control, and hypercoagulability. Given that these tumors exhibit infiltrative growth pattern and are often very large in size complete surgical resection can be challenging but is of vital importance. Even with complete resection, recurrence rates are observed in the range of 65-70% with most in the form of distant metastasis. Adjuvant radiotherapy has been used in an effort to eradicate any remaining microscopic foci of primary tumor completely, reducing the risk of death in margin positive patients by 40% compared to patients who did not receive it1. Dr. Habra also emphasized the importance of Ki-67 expression in risk stratification for determining the most appropriate therapy (see graphic).
Systemic therapy in ACC is directed at cytotoxicity (chemotherapy) and metabolic activity (mitotane). Metastatic ACC carries an extremely poor prognosis with outcomes measured in months. A trial comparing chemotherapy regimens – EDP (etoposide, doxorubicin, cisplatin) v. streptozocin – plus mitotane in each arm did result in an improvement for progression-free survival in the EDP group (median PFS 5.4 mos v. 2.1 mos) but not overall survival (median OS 14.8 mos v. 12.0 mos)2. Various tyrosine kinase inhibitors (TKIs) have been studied in several trials but repeatedly fail to produce any measurable tumor response. One hypothesis for this result, according to Dr. Habra, is the induction of cytochrome p450 activity by mitotane which results in undetectable blood levels of the TKIs. A new trial here at MD Anderson is designed to address this issue using cabozitinib with or without mitotane with close monitoring of drug levels. Looking towards the future, potential therapeutic agents under evaluation right now include IGF1R receptor inhibitors and immunotherapy.
Presented by: Mohammed A. Habra, MD, Department of Endocrine Neoplasia and Hormonal Disorders, University of Texas MD Anderson Cancer Center, Houston, TX, USA
References:
1. Nelson, D.W., S.C. Chang, B.C. Bandera, T.D. Fischer, R. Wollman, and M. Goldfarb, Adjuvant Radiation is Associated with Improved Survival for Select Patients with Non-metastatic Adrenocortical Carcinoma. Ann Surg Oncol, 2018. 25(7): p. 2060-2066.
2. Fassnacht, M., M. Terzolo, B. Allolio, et al., Combination chemotherapy in advanced adrenocortical carcinoma. N Engl J Med, 2012. 366(23): p. 2189-97.
Written by: Justin T. Matulay, MD and Ashish M. Kamat, MD, (@UroDocAsh), Professor, Department of Urology, Division of Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX at the 13th Update on the Management of Genitourinary Malignancies, The University of Texas (MDACC - MD Anderson Cancer Center) November 9-10, 2018, Dan L. Duncan Building, Houston, TX