SCNEC-URO are rare aggressive cancers with limited treatments. Although they frequently co-exist (60-70%) with urothelial carcinoma (UC) at diagnosis, most metastatic biopsies of relapsing patients (pts) show pure small cell (SC) morphology. There are major unmet needs to predict relapse after definitive surgery.
Methods:
Data was extracted from a historical cohort of n=216 pts with surgery for surgically resectable disease (cT1-T4, N0 or N+, M0) at MD Anderson between November 1985 and June 2021. Morphology at resection was defined as: ‘pCR’ (pathological complete response, including no residual carcinoma or carcinoma in situ), ‘Any SCNEC’ (persistence of SC with UC in sample), or ‘Non-SCNEC’ (UC only). Relapse events after surgery were analyzed as time-to-event (TTE) outcomes with competing risk non-parametric methods. Univariable and multivariable analyses identified prognostic factors of relapse.
Results:
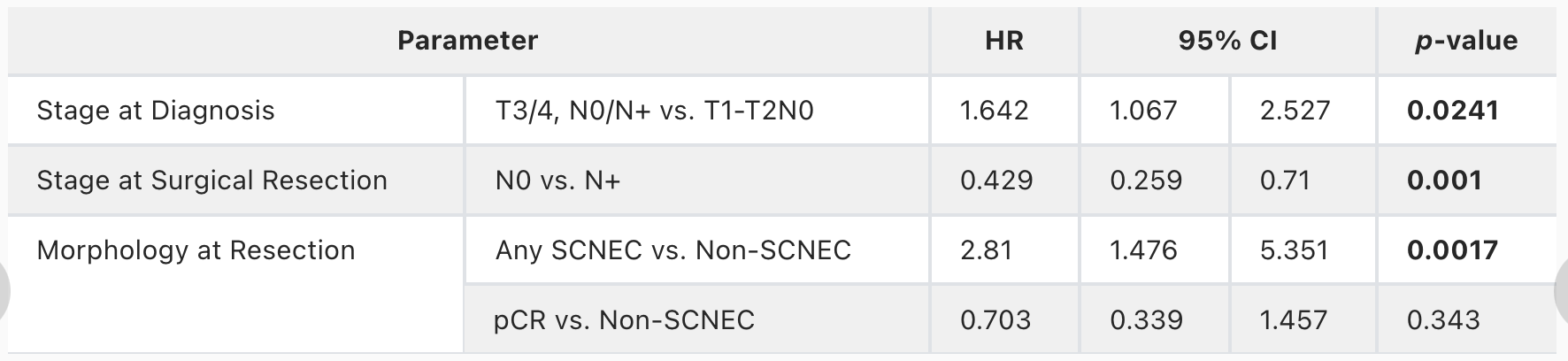
In TTE analysis, cohort events (n=216) included: n=70 censored (alive and relapse-free), n=92 failure events (with relapse), and n=54 competing events (death without known relapse). n=154 (71.3%) received neoadjuvant chemotherapy, including SCNEC regimens in 125/154 (81.2%) and UC regimens in 16/154 (10.4%). The 5-year cumulative incidence function (CIF) of relapse for all pts was 41.92% [95% CI: 35.2% - 48.5%]. CIF rates were significantly different per morphology at resection (Gray’s test, p<.0001). Pts with pCR had the lowest 5-year CIF rate for relapse (18.5%) [11.1% - 27.4%], while pts with ‘Any SCNEC’ had the highest CIF (69.6%) [58.6% - 78.9%]. Pts with Non-SCNEC had an intermediate CIF risk (31.6%) [17.6% - 46.7%]. Staging at resection also showed different CIF rates (Gray’s test, p<.0001). Pts with pT0N0 had the lowest CIF rate (12.8%) [5.6% - 23.2%], with CIF rates increasing with higher staging: pTisN0 (25%) [11.6% - 41%]; pT1N0 (25%) [5.4% - 51.7%]; pT2 or greater, but N0 (52.4%) [41% - 62.7%]. Pts staged node-positive (pN+) did not have an estimated 5-year CIF as most died within 5 years. In multivariable analysis, clinical staging at diagnosis, pathological staging, and cellular morphology at resection were associated with relapse (Table).
Conclusions:
Besides staging at diagnosis and surgery, morphology at resection is a key predictor of relapse. Persistence of the SC component predicts a higher chance of relapse than its eradication and persistence of the UC component. While adjuvant therapy in UC has made significant progress recently, a tailored adjuvant approach addressing the residual SC component at definitive surgery is needed to improve outcomes and decrease relapse.
- Mohammad Jad Moussa, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Nathaniel R. Wilson, Division of Hematology and Oncology, Department of Internal Medicine, University of Michigan, Ann Arbor, MI
- Lianchun Xiao, The University of Texas MD Anderson Cancer Center, Houston, TX
- Georges C. Tabet, Department of Pathology, Division of Pathology and Laboratory Medicine, Houston, TX
- Jianjun Ga, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Amishi Yogesh Shah, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Paul Gettys Corn, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Sangeeta Goswami, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Pavlos Msaouel, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Nizar M. Tannir, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Byron H. Lee, Department of Urology, Division of Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX
- Ashish M. Kamat, Department of Urology, Division of Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX
- Mehrad Adibi, The University of Texas MD Anderson Cancer Center, Houston, TX
- Colin P.N. Dinney, The University of Texas MD Anderson Cancer Center, Houston, TX
- Donna E. Hansel, Department of Pathology, Division of Pathology and Laboratory Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX
- Charles C. Guo, Department of Pathology, Division of Pathology and Laboratory Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX
- Arlene O. Siefker-Radtke, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Matthew T Campbell, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX
- Omar Alhalabi, Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX