BERKELEY, CA (UroToday.com) - Infiltrating (muscle invasive) bladder cancer is the fourth leading cause of cancer death and accounts for 60-90% of all surgically-treated cancers. It is a disease that, even today, is highly problematic -- both in terms of diagnosis and treatment, and in relation to its high incidence and high rates of recidivism, the need for particularly invasive surgery, and to its long-term prognosis.[1] More frequent in males, its likelihood increases with age, with a peak around 65 years, and with growing incidence in developed countries.
To date, radical cystectomy and orthotopic neobladder substitution are the best course of treatment for muscle-invasive bladder cancer without metastases. The surgery involves the removal of the bladder and adipose tissue adhering to it with the neighboring organs (prostate and seminal vesicles in men; uterus, adnexa, and the front of the vagina in women). For the construction of a new bladder, a segment of about 40-60 cm of ileal intestine or colon-sigma, properly configured, is used so as to assume the appearance of a spheroidal cavity to which the ureters are connected.[2, 3] In addition to systemic and local control of the disease, the objective to be achieved is to ensure:
- a good function of the neobladder, namely capacity and adequate voluntary emptying at low pressure
- the recovery of sexual function
- preservation of kidney function
- the limiting of electrolytic and metabolic imbalances, and
- control and ability to treat the development of urinary tract infections that may eventually develop.
Of particular concern in these patients are short-term complications (pyelonephritis and urinary fistulas and enteric), but especially late complications which are likely to occur more than 30 days after placement of the neobladder.[4] Particularly important from the point of view of the nephrologist is the prevention and management of complications of urinary tract infections, hydroureteronephrosis resulting from ureteral obstruction, lithiasis, metabolic acidosis and / or hyperchloraemic, renal insufficiency, and stenosis of the anastomosis neobladder.[5, 6] These clinical situations sometimes occur by themselves, but more often than not in various combinations so as to require either a close collaboration between the urologist and nephrologist, or careful monitoring, especially by ultrasound, in order to preserve as much renal function improvement and at the same time, quality of life.
Ultrasound is already considered to be the primary test of choice in suspected bladder cancer. In the hands of experienced operators, it is useful not only for the relief of the lesion, but also in providing information about tumor staging. Therefore it would be extremely useful to have access to it as a follow up method because it is low cost, repeatable, non-invasive, and risk-free -- with high sensitivity and specificity, even in patients with orthotopic neobladders (Figures 1 and 2).

Figure 1

Figure 2
Early in the post-surgical period, patients with urinary diversions should be assigned to a nephrologist for morphological and functional assessment of the urinary tract. In addition to oncological follow-up (for a period of 5 years) for the possible recurrence of the disease, in patients with orthotopic neobladder, there must be integrated ongoing follow-up that includes the monitoring of renal function and metabolic alterations, the morphological evaluation of renal function, the urinary tract, and the tank.[7] There are no studies in the literature regarding timing and mode of follow-up. Particularly in the post-operative period, the reconstructed neobladder, unlike the natural one, favors the loss of water and salts. In patients with normal renal function, the controls on renal function, the fluid and electrolyte balance, and acid-basic balance should be monitored on a monthly basis in the first 6 months after surgery, then every 3 months for a further 2 years, and on an ongoing basis every 6 months thereafter. Often, these patients present an early impairment of renal function, sometimes independent of hydronephrosis, due to chronic infection of the urinary tract, ureteral obstruction, and / or high pressures of the neobladder. The frequency of inspection in such patients should be personalized according to the degree of renal insufficiency. In fact, in some cases, renal failure may be so severe as to require dialysis.
Equally, ultrasound monitoring should be carried out every 2 months to measure morphological renal parenchymal thickness, as well as detect any expansion of the upper urinary tract, to recognize hydronephrosis (Figure 3), the presence of stones (Figures 4 and 5) and/or residual post-void urinary retention.[8] The dilation of the urinary tract ranges from simple pyelectasis to hydronephrosis of a marked degree (grade III-IV). Urinary stones may form either as a result of acidosis hyperchloraemic, residual post-void urine, urinary infections, as well as from the non-removal of the metal clips not fully covered by the mucous membrane, a basis for the possible formation of a nucleus of aggregation.
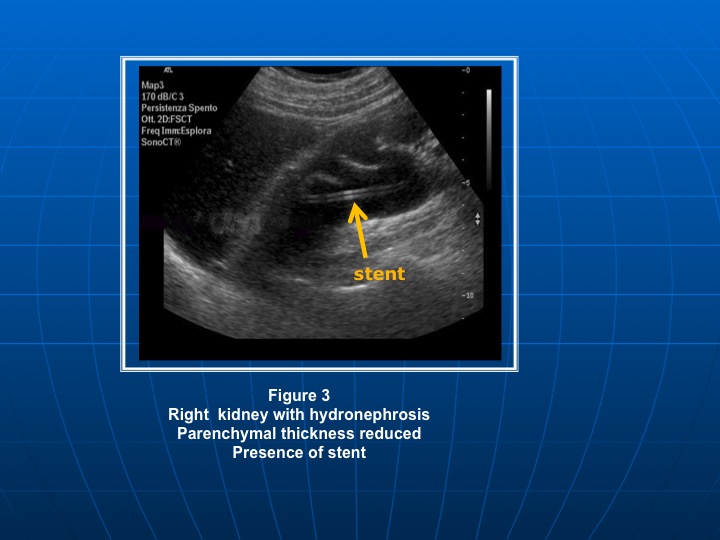
Figure 3

Figure 4

Figure 5
The stenosis of the anastomosis uretero-neobladder, mainly caused by ischemia of the end portion of the ureter or a tumor recurrence, is the most dangerous complication as it results in a degradation of renal function.[9, 10] Therefore we propose an approach that allows to correct both the early metabolic abnormalities, particularly hypokalemia and acidosis, related to the reabsorption of electrolytes from the intestinal tract used for the tank, and the hydronephrosis due to stenosis of the anastomosis uretero-neobladder (for which it becomes necessary to entrust the patient to the urologist for correction (replacement of stents and / or positioning of any nephrostomy))(Figures 6 and 7).

Figure 6

Figure 7
In view of the significant negative impact on the quality of life of patients (loss of urinary continence, altered body image, impairment of sexual function, etc.), European guidelines recommend periodic blood chemistry assessments of the morphological and functional characteristics of the urinary tract.[11]
Hence a multidisciplinary approach is required, with the predominant role falling to the nephrologist who assumes the responsibility and management of these patients in order to detect early onset of complications -- and undertakes a custom treatment. The nephrologist is able to identify the potential nephrotoxicity of some drugs and limit the possibility of existing sequelae from causing irreversible damage.
References:
- Abdel-Latif M, Abol-Enein H, El-Baz Mahmoud, Ghoneim M.Nodal involvement in bladder cancer cases treated with radical cystectomy:incidence and prognosis. J Urol 2004;172:85-89
- R.E. Hautmann, “Urinary diversion: ileal conduit to neobladder”, J Urol 2003 vol 169, no3,pp.834-842
- D.J Gallagher and M.I. Milowsky, “Bladder cancer” Current Treatment Options in Oncology, vol 10, no. 3-4, pp. 205-215, 2009
- Buscarini M, Pasin E, Stein JP: Complications of radical cystectomy. Minerva Urol Nefrol 2007 Mar;59(1):67-87
- Andrea G. Lanz, MD; M. Eric Saltel, MD,FRCSC; Ilias Cagiannos, MD, FRCSC Renal and functional outcomes following cystectomy and neobladder reconstruction CUAJ 2010 October vol 4 issue 5
- Hautmann RE, De Petriconi RC, Volkmer BG 25 years of experience with 1000 neobladders: long-term complications J Urol. 2011 Jun;185(6):2207-12
- BG Wolkmer, R Kuefer, GC Bartsch, et al Oncological follow up after radical cystectomy for bladder cancer is there any benefit? J Urol Vol 181,1587-1593, Aprile 2009llow-up. BJU International 2009 105, 860-863
- A. Mudoni, F. Caccetta, M. Caroppo, F. Musio, A. Accogli, A. Noce, E. Ferramosca, V. Nuzzo: Role of ultrasound in management of long-term complications after to radical cystectomy and orthotopic neobladder construction: case report Archivio Italiano di Urologia e Andrologia Vol 84;n 4 December 2012
- Mattew K.Tollefson, Daniel S. Elliott, Horst Zincke and Igor Frank Long-term outcome of ureterosigmoidostomy: an anlysis of patients with > 10 years of follow-up. BJU International 2009 105, 860-863
- LCE Martin, U Abah, E Bean, S Gupta Metabolic acidosis: neo-considerations for general surgeons. Ann R Coll Surg Engl 2012;94:e249-e250
- Babjuk M, Oosterlinck W, Sylvester R, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder. Eur Urol 2008;54:303314
Written by:
Anna Mudoni,a Francesco Caccetta,a Maurizio Caroppo,a Fernando Musio,a Antonella Accogli,a Maria Dolores Zacheo,a Domenica Burzo,a Giancamillo Carluccio,b and Vitale Nuzzoa as part of Beyond the Abstract on UroToday.com. This initiative offers a method of publishing for the professional urology community. Authors are given an opportunity to expand on the circumstances, limitations etc... of their research by referencing the published abstract.
aU.O. Nephrology and Dialysis, Hospital “Cardinale G. Panico”, Tricase, Lecce, Italy
bU.O. Urology Hospital “Cardinale G. Panico”, Tricase, Lecce, Italy
![]()
More Information about Beyond the Abstract