BERKELEY, CA (UroToday.com) - Our case report showed a positive effect of modern external beam radiotherapy as volumetric modulated arc therapy (VMAT) for lymph-node-positive prostate cancer.[1] The patient had salvage VMAT because a PET/CT had shown a pelvic lymph node metastasis.
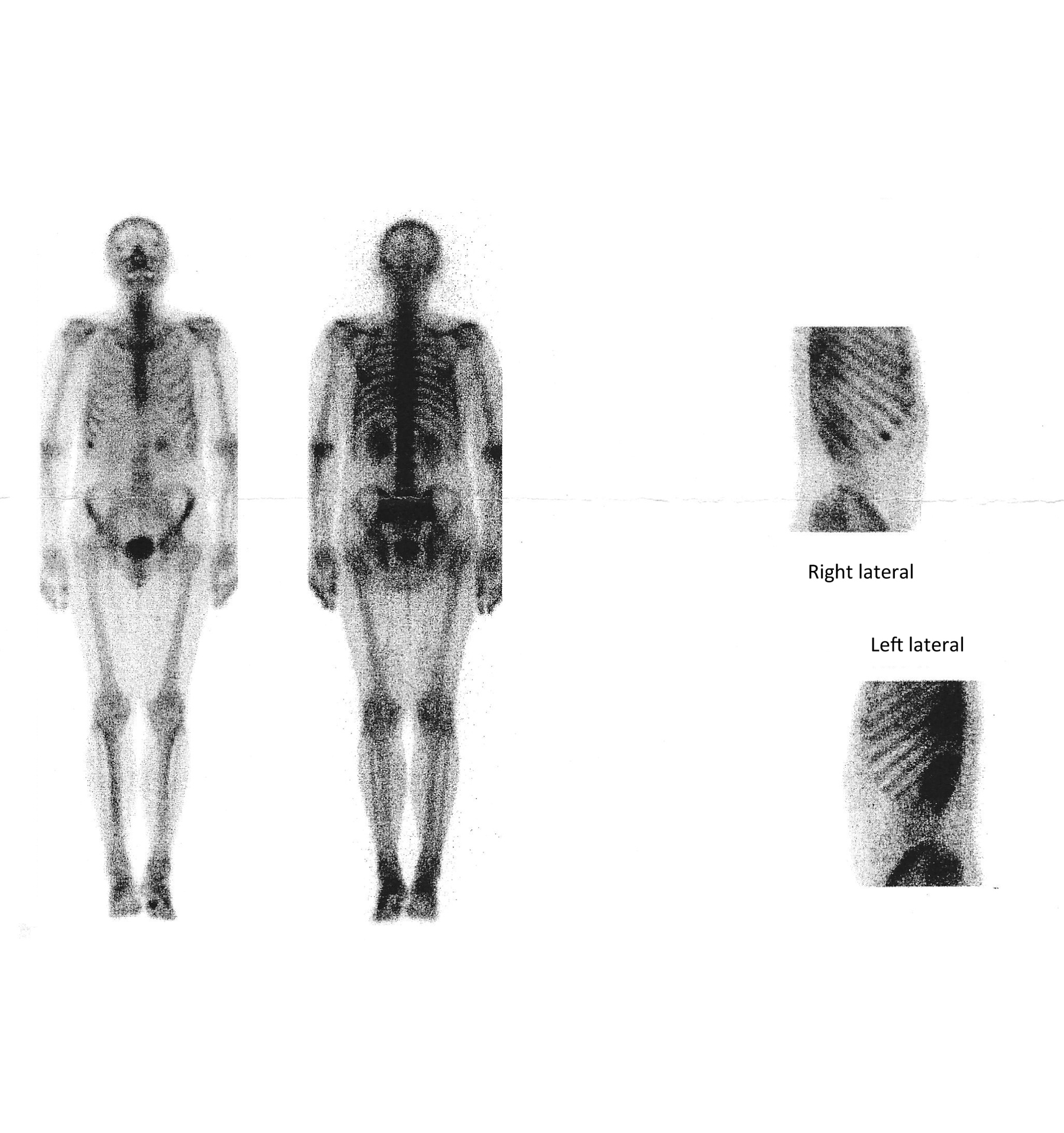
ln 2007, our patient underwent a radical prostatectomy. Limited pelvic lymph node dissection showed macro-metastases in 3 of 6 left lymph nodes. He had adjuvant androgen deprivation therapy (ADT), and PSA declined to unmeasurable levels in the first year of treatment. Shortly afterwards, he had a rise of PSA as biochemical recurrence. He had a Tc99m methylene diphosphate bone scan. It showed high uptakes in a rib and a toe (Figure 1) but the uptakes reflected healing fractures. Similarly, the European Association of Urologists (EAU) discourages that patients with PSA < 20 ng/ml undergo bone scans,[2] He was treated with denosumab, a treatment that significantly prolongs bone-metastasis-free survival.[3]
In June 2011, our patient underwent an anti-1-amino-3-18[F]-fluorocyclobutane-1-carboxylic acid (FACBC) PET/CT scan with a PSA of 1.1 ng/ml. The PET/CT scan showed a metastasis in a pararectal lymph node (Figure 2). When patients with biochemical recurrence have PSA >1.0 ng/ml, a PET/CT scan with an adequate tracer is likely to detect the anatomy of a positive uptake.[4] For patients with PSA between 1 and 5 ng/ml, a positive PET/CT scan most often points to loco-regional lesions. Most U.S. PET/CT scans for prostate cancer use 18[F]-fluoro-3-deoxy-D-glucose (FDG) as tracer, and the scans have a proven value for treatment.[5] However in a recent meta-analysis, choline PET/CT scans gave positive findings twice as often as FDG PET/CT scans.[4] Two studies of PET/CT scans found that FACBC was an even better tracer than choline.[6, 7]
We used the PET/CT scan for planning of the radiotherapy. VMAT included both the metastatic lymph node and the other pelvic lymph nodes. They were included because a positive PET/CT may not reveal the full extent of metastases in pelvic lymph nodes.[8] The radiotherapy gave a partial remission for 16 months and limited toxicity from organs at risk. Nevertheless, radiotherapy for node-positive prostate cancer remains for debate. Studies based on the Surveillance, Epidemiologic, and End Results (SEER) database showed that unspecified adjuvant radiotherapy did not improve overall survival.[9, 10] In contrast, Briganti et al. found increased overall survival when they gave adjuvant radiotherapy after a radical prostatectomy and ADT.[11] EAU recommends that node-positive patients are treated with adjuvant radiotherapy.[2] Salvage radiotherapy also had positive effects for series of patients with node-positive disease.[12]
EAU guidelines recommend to institute radiotherapy for a biochemical recurrence while PSA is < 0.5 ng/ml. They also recommend to use the prostate bed as treatment target if a patient has a known local recurrence.[2] However, for patients with PSA < 0.5 ng/ml, imaging modalities rarely show positive findings. So PET/CT examinations should wait until PSA is > 1.0 ng/ml if treatment should be based on positive findings. A randomized trial for patients with biochemical recurrence may examine whether it is best to include, or not to include, PET/CT scans in the diagnostic work-up (Figure 3).
 |
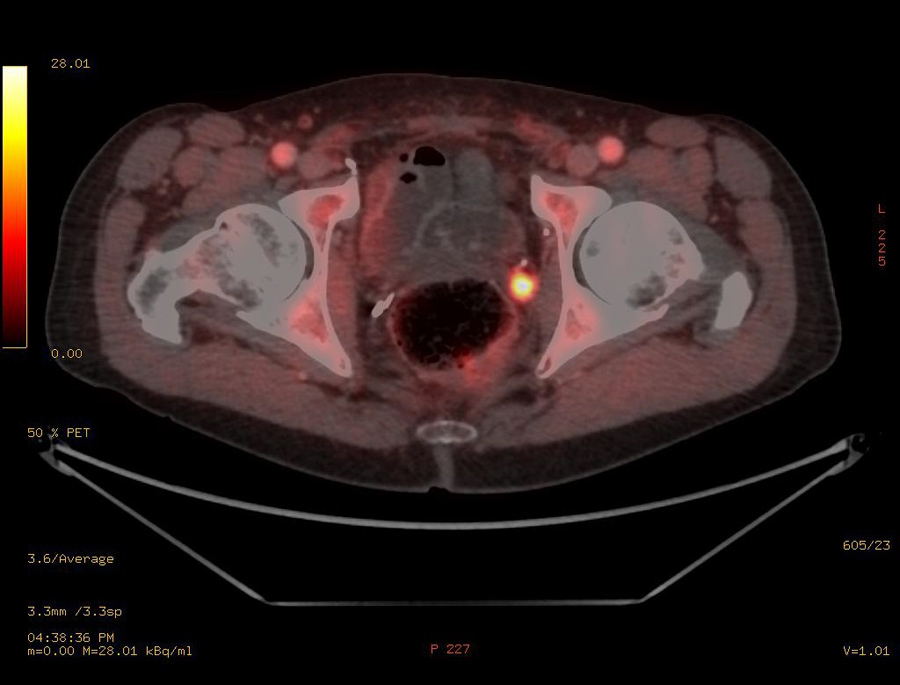 |
| Figure 1. A Tc99m methylene diphosphate bone scan showed false-positive high uptakes in the tenth right rib and the first toe. | Figure 2. The anti-1-amino-3-18[F]-fluorocyclobutane-1-carboxylic acid (FACBC) PET/CT scan showed a high uptake in a pararectal lymph node. |
 |
|
| Figure 3. Proposal for a trial for biochemical recurrence of prostate cancer randomized to management with or without PET/CT scans. |
References:
- FE von Eyben, A Kangasmaki, T Kiljunen, T Joensuu, "Volumetric-modulated arc therapy for a pelvic lymph node metastasis from prostate cancer: a case report," Tumori 99: (May-Jun 2013): e120-3.
- A Heidenreich, PJ Bastian, J Bellmunt, M Bolla, S Joniau, T van der Kwast, et al., "EAU Guidelines on Prostate Cancer. Part II: Treatment of Advanced, Relapsing, and Castration-Resistant Prostate Cancer," European Urology 65: (Feb 2014): 467-79.
- MR Smith, F Saad, S Oudard, N Shore, K Fizazi, P Sieber, et al., "Denosumab and bone metastasis-free survival in men with nonmetastatic castration-resistant prostate cancer: exploratory analyses by baseline prostate-specific antigen doubling time," Journal of Clinical Oncology 31: (Oct 20 2013): 3800-6.
- FE von Eyben, K Kairemo, "Meta-analysis of 11C-choline and 18F-choline PET/CT for management of patients with prostate cancer," Nuclear Medicine Communications 35: (Mar 2014): 221-30.
- BE Hillner, BA Siegel, L Hanna, AF Shields, F Duan, IF Gareen, et al., "Impact of 18F-FDG PET used after initial treatment of cancer: comparison of the National Oncologic PET Registry 2006 and 2009 cohorts," Journal of Nuclear Medicine 53: (May 2012): 831-7.
- C Nanni, R Schiavina, S Boschi, V Ambrosini, C Pettinato, E Brunocilla, et al., "Comparison of 18F-FACBC and 11C-choline PET/CT in patients with radically treated prostate cancer and biochemical relapse: preliminary results," European Journal of Nuclear Medicine and Molecular Imaging 40 Suppl 1: (Jul 2013): S11-7.
- R Schiavina, S Concetti, E Brunocilla, C Nanni, M Borghesi, G Gentile, et al., "First Case of F-FACBC PET/CT-Guided Salvage Retroperitoneal Lymph Node Dissection for Disease Relapse after Radical Prostatectomy for Prostate Cancer and Negative C-Choline PET/CT: New Imaging Techniques May Expand Pioneering Approaches," Urologia Internationalis: (Dec 7 2013).
- NM Passoni, N Suardi, F Abdollah, M Picchio, G Giovacchini, C Messa, et al., "Utility of [(11)C]choline PET/CT in guiding lesion-targeted salvage therapies in patients with prostate cancer recurrence localized to a single lymph node at imaging: Results from a pathologically validated series," Urologic Oncology 32: (Jan 2014): 38 e9- e16.
- PA Johnstone, V Assikis, M Goodman, KC Ward, RH Riffenburgh, V Master, "Lack of survival benefit of post-operative radiation therapy in prostate cancer patients with positive lymph nodes," Prostate Cancer and Prostatic Diseases 10: 2007): 185-8.
- JR Kaplan, KJ Kowalczyk, T Borza, X Gu, SR Lipsitz, PL Nguyen, et al., "Patterns of care and outcomes of radiotherapy for lymph node positivity after radical prostatectomy," BJU International 111: (Jun 2013): 1208-14.
- A Briganti, RJ Karnes, LF Da Pozzo, C Cozzarini, U Capitanio, A Gallina, et al., "Combination of adjuvant hormonal and radiation therapy significantly prolongs survival of patients with pT2-4 pN+ prostate cancer: results of a matched analysis," European Urology 59: (May 2011): 832-40.
- F Casamassima, L Masi, C Menichelli, I Bonucci, E Casamassima, M Lazzeri, et al., "Efficacy of eradicative radiotherapy for limited nodal metastases detected with choline PET scan in prostate cancer patients," Tumori 97: (Jan-Feb 2011): 49-55.
Written by:
Finn Edler von Eyben, Aki Kangismäki, Timo Kiljunen, and Timo Joensuu as part of Beyond the Abstract on UroToday.com. This initiative offers a method of publishing for the professional urology community. Authors are given an opportunity to expand on the circumstances, limitations etc... of their research by referencing the published abstract.
Center of Tobacco Control Research, Odense, Denmark
Docrates Comprehensive Cancer Center, Helsinki, Finland
Corresponding Author: Finn Edler von Eyben, Birkevej 17, DK-5230 Odense M, Denmark, e-mail:
More Information about Beyond the Abstract