Renal cell carcinoma (RCC) accounts for 2% of all cancers. Although it often results in lung metastasis, bony metastases are uncommon. RCC may not be diagnosed until after it has metastasized because the primary tumor can grow fairly large without creating symptoms such as flank pain or a mass in the abdomen. We report a 38-year-old male who presented with right loin pain typical of ureteric colic. Clear cell RCC was not diagnosed until histological evaluation was completed after a nephrectomy. A bone scan showed widespread skeletal metastasis. Use of bone scans and other diagnostic tests for suspected RCC is discussed.
KEYWORDS: Renal cell cancer; Diagnosis; Bone scan; Treatment.
CORRESPONDENCE: Daben Dawam, 8 Hilton Road, Cliffe Woods, Rochester, Kent ME3 8LA, England ().
CITATION: UroToday Int J. 2011 Apr;4(3):art25. doi:10.3834/uij.1944-5784.2011.06.01
ABBREVIATIONS AND ACRONYMS: CT, computed tomography; ECOG, Eastern Cooperative Oncology Group; RCC, renal cell carcinoma.
INTRODUCTION
Renal cell carcinoma (RCC) accounts for 2% of all cancers. Although it often results in lung metastasis, bone metastases are uncommon. However, when bone metastasis occurs, it is the second most common site after the lung [1]. RCC may not be diagnosed until after it has metastasized because the primary tumor can grow fairly large without creating symptoms such as flank pain or a mass in the abdomen.
There are few case reports describing clear RCC and bone metastasis in the literature. In the present case, the RCC was not diagnosed immediately because a ureteric stone was suspected. Therefore, tests that would have revealed the RCC were not chosen during the early diagnostic period.
CASE REPORT
A 38-year-old male presented with right loin pain typical of ureteric colic. He had diabetes mellitus and was dependent on insulin. There was no known history of urinary stones or positive family history. His temperature was 38°C.
Intravenous urography (IVU) did not show any radiopaque shadows on the plain film that would suggest a stone. Subsequent contrast studies demonstrated mild hydronephrosis. The patient also had microscopic hematuria. The clinical diagnosis was a possible ureteric stone; a stent was inserted. He stabilized and went home with the intention of a planned ureteroscopy and possible removal of a stone.
One week later, the patient returned. He was still in pain. Stent irritation was suspected, so the stent was removed. Because he was septic on this readmission, he had an abdominal ultrasound. The ultrasound showed a stone in the lower pole of the right kidney with solid components. An abscess was considered a possibility, but a sinister lesion could not be ruled out. A technetium dimercaptosuccinic acid (DMSA) scan showed a nonfunctioning area that was thought to represent infected devitalized tissue. Computed tomography (CT) guided aspiration cytology showed atypical cells. Urine cytology showed leucocytes and occasional urothelial cells but no malignant cells. Blood and urine cultures did not show any growth. Serum urea and electrolytes were normal; white cell count was 16.7 x 109/L, hemoglobin was 11.0 g/dL, and platelets were 676,000 x 109/L. Magnesium was 0.90 mmol/L, calcium was 1.90 mmol/L, and albumin was 23 g/dL.
The patient was deteriorating quickly, despite attention to diabetes control and antibiotic treatment for sepsis. He looked ill and was losing weight. He was prepared for nephron-sparing surgery, with the possibility of radical nephrectomy depending on the intraoperative finding. We used a transperitoneal approach and completed a nephretomy ( ). He made an uneventful recovery and went home after 7 days.
). He made an uneventful recovery and went home after 7 days.
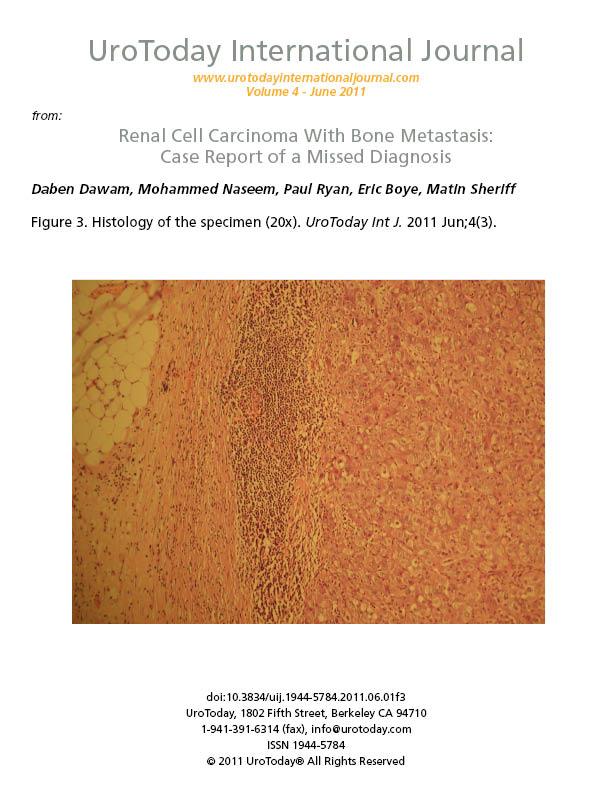
Histology of the nephrectomy specimen showed clear cell RCC ( ;
;  ). The patient was readmitted with vomiting, back pain, rapid weight loss, and dehydration. A bone scan (
). The patient was readmitted with vomiting, back pain, rapid weight loss, and dehydration. A bone scan ( ) showed widespread skeletal metastasis. Palliative care was given and he died in hospice care 1 month after surgery.
) showed widespread skeletal metastasis. Palliative care was given and he died in hospice care 1 month after surgery.
DISCUSSION
A bone scan is not routinely requested before surgery for RCC [2]; it is typically reserved for patients with suspected spread of cancer outside the kidney. A scan is indicated in the presence of symptoms of bone pain or elevation of serum enzymes of alkaline phosphatase or calcium levels. Patients with early RCC often do not undergo a routine bone scan unless they have bone pain; patients with advanced RCC often have routine bone scans, particularly prior to surgery. Other diagnostic tests for suspected RCC include CT or axial magnetic resonance imaging (MRI) of the abdominal area.
Researchers have been evaluating ways to determine which patients are at a high risk for having bone metastases so that only those patients would undergo a bone scan. In a recent study [3], the authors studied which variables may be indicative of bone metastases in patients diagnosed with RCC. This study included a database of 1,357 patients who underwent treatment that included surgery for RCC at a single institution. The data were reviewed in an attempt to find associations between specific variables and the presence of bone metastases. Of these patients, 37% had metastases and 14% had bone metastases. Of all patient variables assessed (including the extent of the cancer, metastases to other areas of the body, enzyme levels that may be indicative of cancer spread, and symptoms of the muscular and skeletal systems), only a patient's score on the Eastern Cooperative Oncology Group (ECOG) performance status scale was indicative of bone metastases. Patients with a performance status of 0 (completely ambulatory with no symptoms that inhibit daily activities) had only a 1.4% incidence of bone metastasis, regardless of all other variables. However, patients with an ECOG performance status > 0 had significantly higher rates of bone metastases. The researchers concluded that ECOG performance status scores are highly predictive of bone metastasis in patients diagnosed with RCC. Patients with an ECOG performance status > 0 may benefit from a bone scan during their diagnostic work-up or prior to surgery. The authors concluded that patients diagnosed with RCC may wish to speak with their physicians about their individual risks and benefits of undergoing a bone scan.
Would a positive preoperative bone scan have altered our management of the present case? The answer is yes, although CT or axial MRI of the abdomen may also have shown the extent of the carcinoma. Surgery is still an option in the presence of metastases, but this patient had such widespread metastases that surgery was unlikely to be beneficial.
FIGURES
REFERENCES
- Parada SA, Franklin JM, Uribe PS, Manoso MW. Renal cell carcinoma metastases to bone after a 33-year remission. Orthopedics. 2009;32(6):446. PubMed; CrossRef
- Koga S, Tsuda S, Nishkido M, et al. The diagnostic value of bone scan in patients with renal cell carcinoma. J Urol. 2001;166(6)2126-2128. PubMed; CrossRef
- Shvarts O, Lam JS, Kim HL, Han KR, Figlin R, Belldegrun A. Eastern Cooperative Oncology Group performance status predicts bone metastasis in patients presenting with renal cell carcinoma: implication for preoperative bone scans. J Urol. 2004;172(3):867-870. PubMed; CrossRef