Meeting: 2023 American Society for Therapeutic Radiation Oncology (ASTRO) 65th Annual Meeting
Date: October 1st – October 4th, 2023
Session: Personalization of Systemic Therapy for Localized to Metastatic Prostate Cancer
Presentation Title: Duration and Combination of Systemic Therapies for Patients with Very High Risk, Node Positive, and Oligometastatic Prostate Cancer
The 2023 American Society for Therapeutic Radiation Oncology (ASTRO) 65th Annual Meeting
held in San Diego, CA between October 1st and 4th, 2023 was host to a session on miscellaneous genitourinary topics. Dr. Anne Rajkumar discussed the duration and combination of systemic therapies for patients with very high-risk, node positive, and oligometastatic prostate cancer.
Dr. Rajkumar began by presenting a case of a 56-year-old male with Gleason score 4+5=9 disease, PSA 5.1 ng/ml, and with evidence of extraprostatic extension on imaging. His PSMA-PET was negative for regional and distant disease. He declined surgery in favor of radiation therapy. Given his NCCN high-risk classification, what are considerations for his hormone therapy?
Currently, concurrent androgen blockade is recommended for patients with unfavorable intermediate risk or worse disease. The duration of concurrent ADT varies from 6 months to 2 years in the high-risk patients.
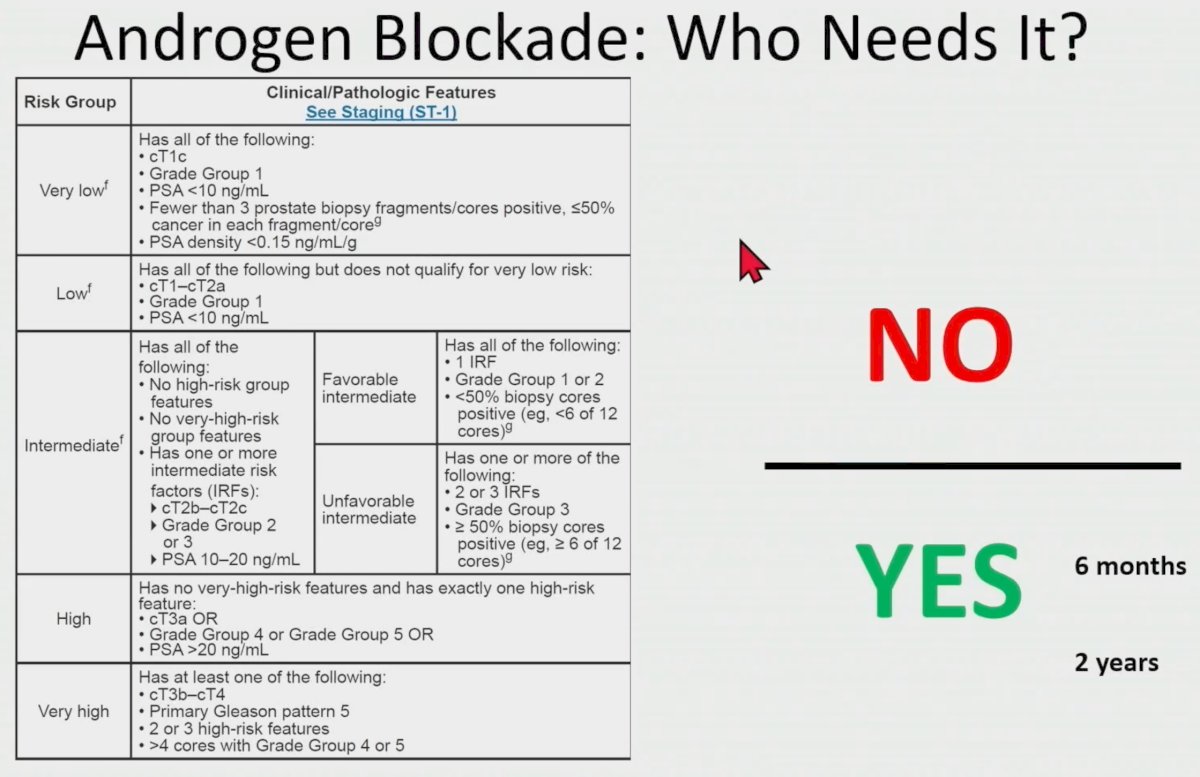
But which patients might benefit from additional androgen blockade in the form of an ‘ADT doublet’ with the addition of an androgen receptor pathway inhibitor such as abiraterone, enzalutamide, apalutamide, or darolutamide? At the current time based on the available evidence, this practice should be reserved for patients with NCCN very-high risk disease, particularly those with 2 or 3 high-risk features (cT3-4, Grade Group 4-5, PSA ≥40 ng/ml).
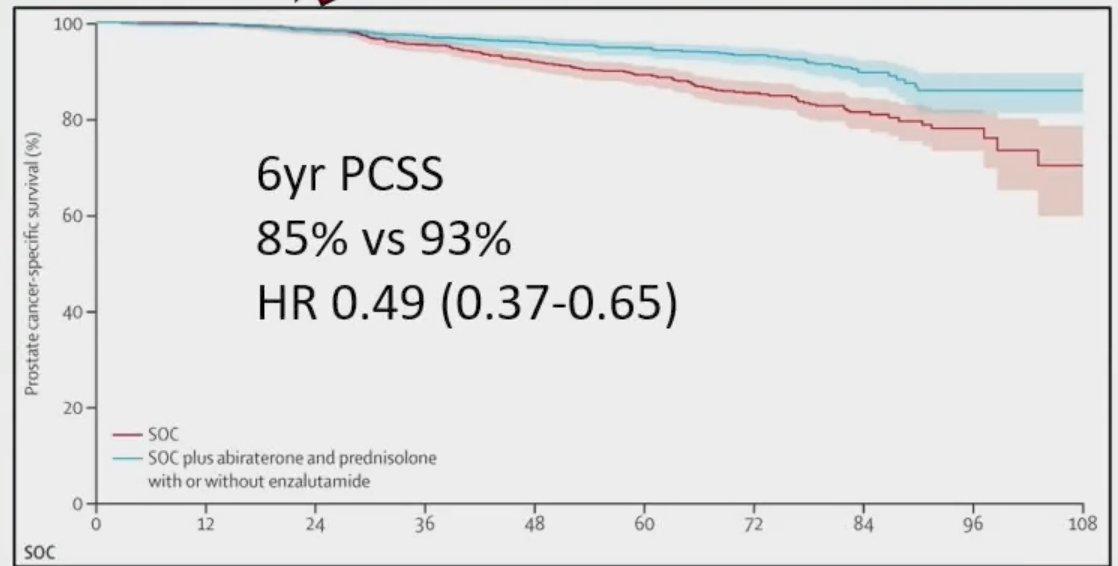
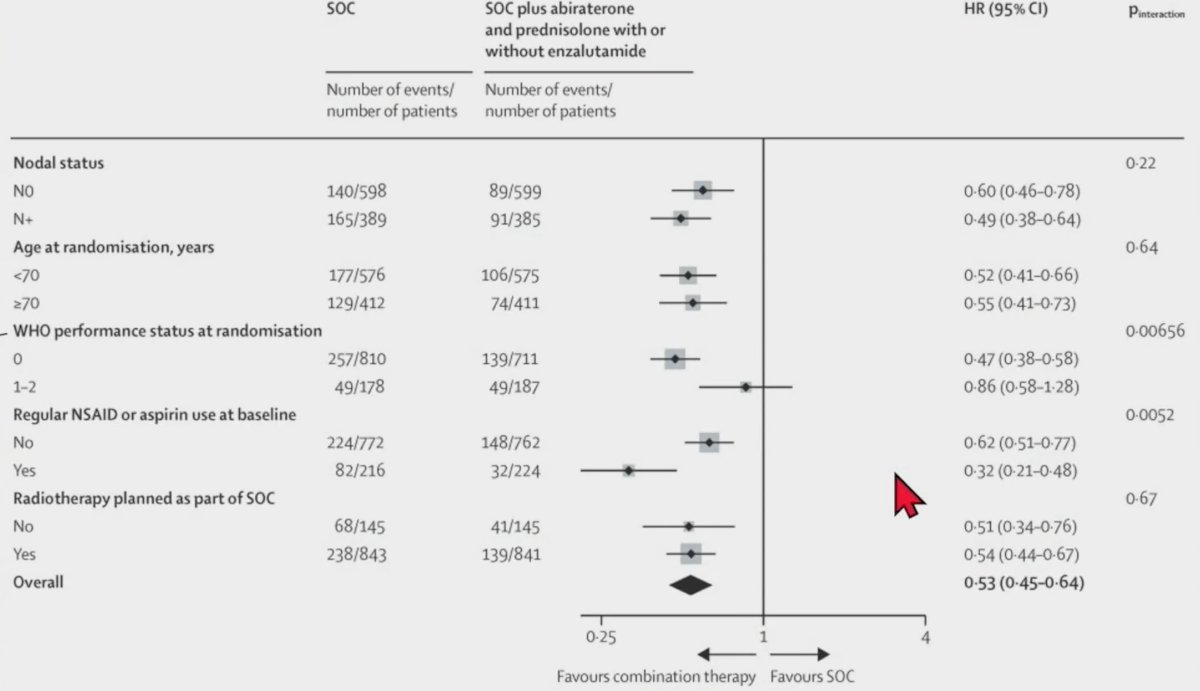
This recommendation is based on results of a STAMPEDE meta-analysis1 that demonstrated that the addition of abiraterone 1,000 mg daily + oral prednisolone (5 mg daily) +/- enzalutamide for a median of 20 – 24 months to ADT in patients with high-risk disease (defined as node positive, or, if node negative, having at least two of the following: tumour stage T3 or T4, Gleason sum score of 8–10, and PSA concentration ≥40 ng/mL) or high-risk relapse was associated with significant improvements in:
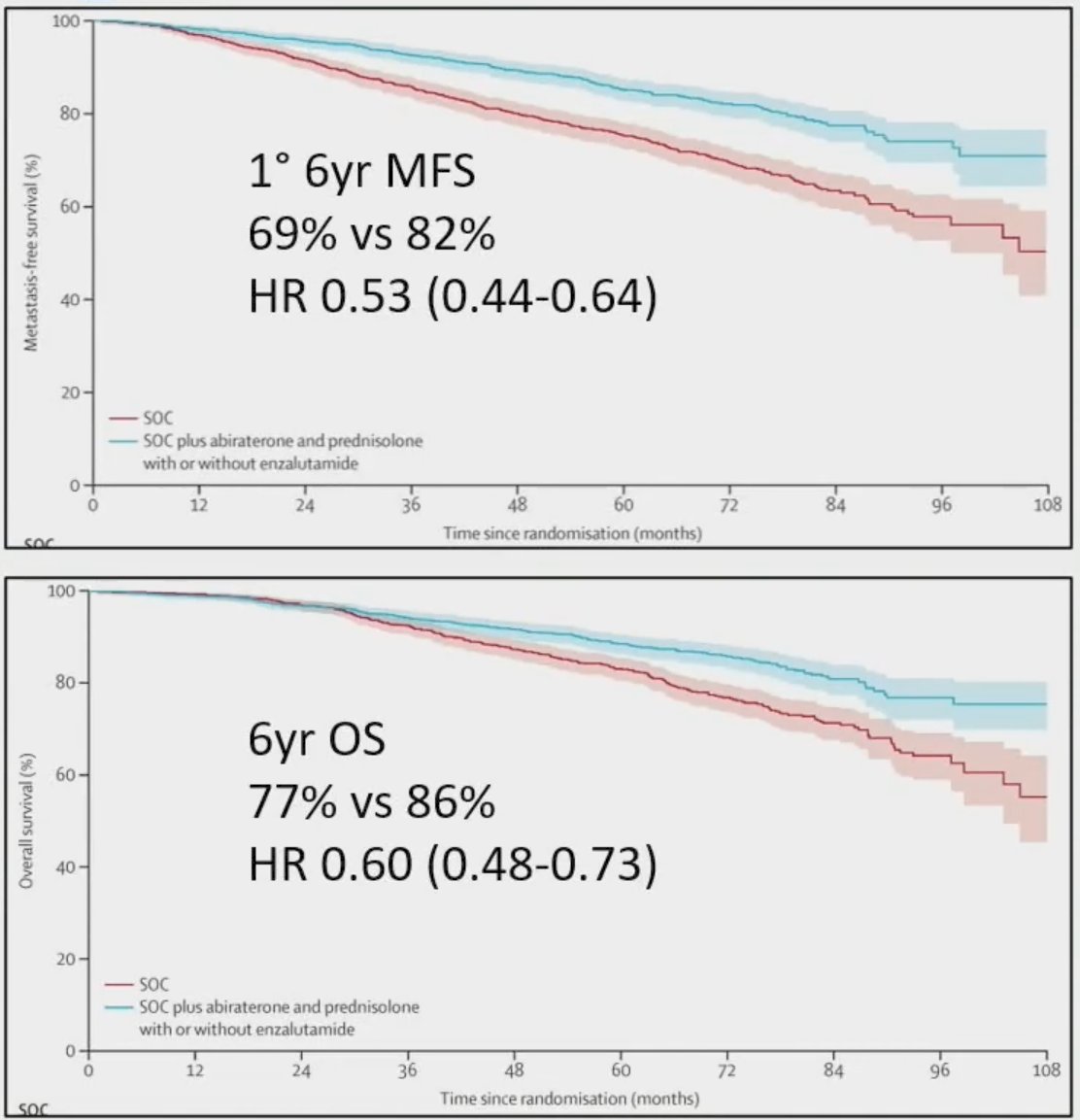
- Metastasis-free survival (HR: 0.53, 95% CI: 0.44 – 0.64)
- Prostate cancer-specific survival (HR: 0.49, 95% CI: 0.37 – 0.65)
- Overall survival (HR: 0.60, 95% CI: 0.48 – 0.73)
Dr. Rajkumar emphasized that there was significant clinical heterogeneity among patients in this study cohort, which has significant implications for the external validity/generalizability of the study results and their applicability to patients in her clinical practice. Patient age ranged from 43 to 86 and the PSA interquartile range varied between 15 and 75 ng/ml. However, 75% of patients had Gleason score 8 – 10 and 90% had cT3-4 disease. As such, in her opinion, these are the two most reliable clinical variables to recommend abiraterone use in this setting. As such, returning to the case presentation, given the patient’s Gleason score 9 disease and presence of extraprostatic extension on imaging (i.e., cT3), the patient received long-term leuprolide and abiraterone/prednisolone along with his definitive radiotherapy.
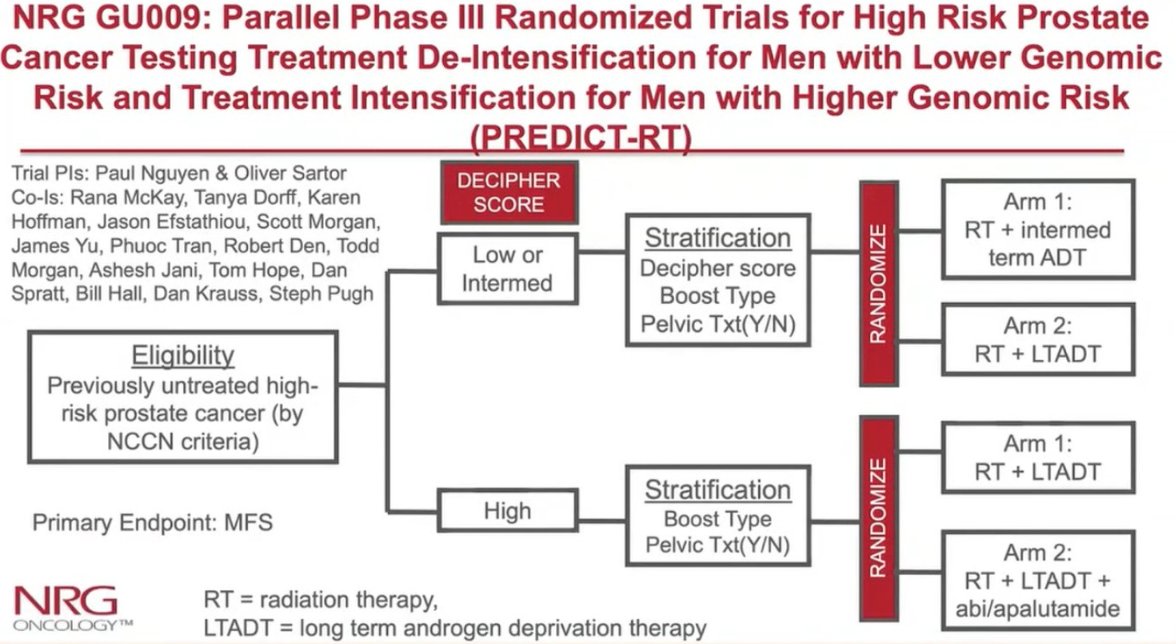
However, do all patients with high-risk disease need long-term ADT (e.g., 24 months) and can we use an alternate androgen receptor pathway inhibitor, such as apalutamide? Furthermore, what about patients with node negative disease on conventional imaging who may be PSMA positive? The NRG GU-009 study (PREDICT-RT) will attempt to address these questions. This study has 2 components:
- De-Intensification component: To determine whether men with NCCN high risk prostate cancer who are in the lower 2/3 of Decipher genomic risk (< 0.85) can be treated with 12 months ADT plus RT instead of 24 months ADT+RT and experience non-inferior metastasis-free survival.
- Intensification component: To determine whether men with NCCN high risk prostate cancer who are in the upper 1/3 of Decipher genomic risk (> 0.85) or have node-positive disease by conventional imaging (MRI or CT scan) will have a superior metastasis-free survival (MFS) through treatment intensification with apalutamide added to the standard of RT plus 24 months ADT.
Patients will be study eligible if they have node positive disease on conventional imaging or have just one high-risk feature (PSA >20 ng/ml, Gleason score 8 – 10, cT3-4 on MRI). Patients will be allowed to undergo a PSMA-PET/CT, per the treating physician’s discretion. Furthermore, if positive, apalutamide may become an additional treatment option in this setting.
Next, Dr. Rajkumar presented a 2nd case of a 73-year-old male with Gleason score 4+3=7 with cribriform glands, PSA 6.3 ng/ml, and high-risk features with evidence of extraprostatic extensions with likely bladder involvement and seminal vesicle invasion on MRI. A PSMA-PET was obtained and showed mild-moderate activity in 3 nodes (0.7 cm L external iliac, 0.5 cm R common iliac, and 0.4 cm R obturator node), none of which meet the criteria for involvement on conventional imaging. Dr. Rajkumar asked: What are considerations for his hormone therapy?
Based on subgroup analysis of the STAMPEDE meta-analysis, it appears that there is an additional benefit to addition of abiraterone to ADT in patients with excellent performance status.
As such, Dr. Rajkumar argued that in select healthy patients, with evidence of locally aggressive disease (based on extent of extraprostatic extension), with multiple borderline positive nodes >3-5 mm, with a disproportionately low PSA given the extent of disease (increased risk of de-differentiated disease), she will consider shorter-term abiraterone addition for 12 months, compared to the 20 – 24 months in the STAMPEDE trial.
Next, Dr. Rajkumar transitioned to the use of hormone therapy in the salvage radiotherapy setting. She presented a 3rd case of a 58-year-old male with Gleason score 4+3=7, with a PSA of 10.5 ng/ml, and evidence of extraprostatic extension and seminal vesicle invasion on MRI. PSMA-PET showed minimally avid bilateral external iliac nodes, “favored to be reactive”. He had significant lower urinary tract symptoms, and thus chose to proceed with surgery that demonstrated:
- Gleason score 4+5=9 with invasion of the bladder, seminal vesicle, and extraprostatic tissues, with negative margins, and 3/20 lymph nodes positive
His post-operative PSA was 0.6 ng/ml and rose to 1.5 ng/ml within 3 months. A post-operative PSMA PET showed a 4 cm external iliac lymph node with possible lymphocele component. Would this patient benefit from ADT in the salvage setting?
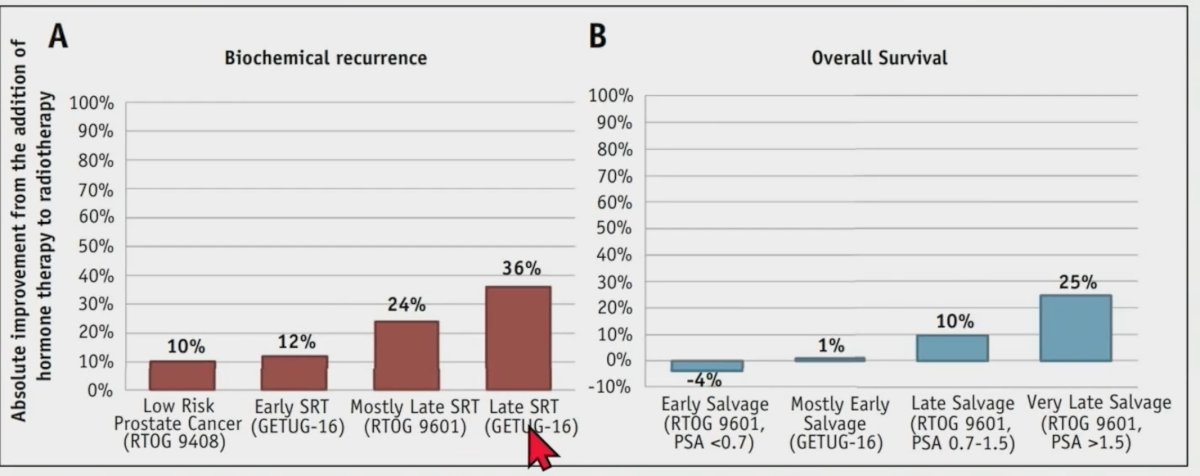
Based on evidence from GETUG-AFU-16 and RTOG 9601, it appears that patients with a PSA ≥0.7 ng/ml derive a benefit, and this is most notable in patients receiving ADT in the “late” salvage radiotherapy setting as demonstrated in panel A below:
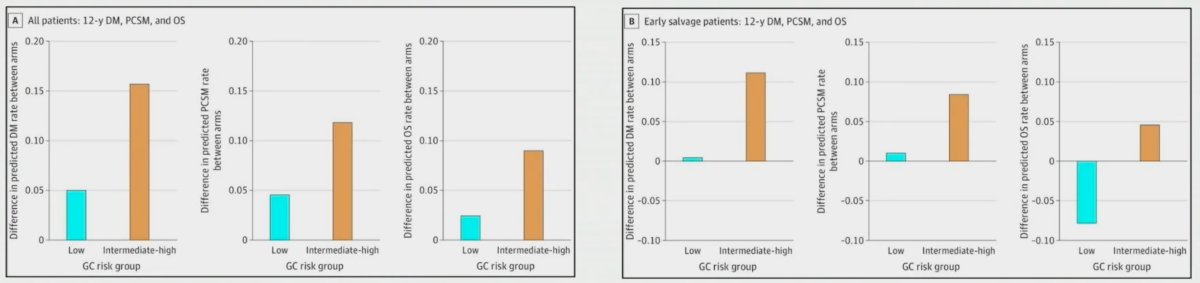
Another consideration in this setting may be the use of the genomic classifier Decipher®. This is especially useful for patients planned for ADT in the early salvage setting (PSA <0.7 ng/ml), with patients having a low Decipher® score having worse overall survival outcomes when ADT is added to the salvage radiotherapy.2
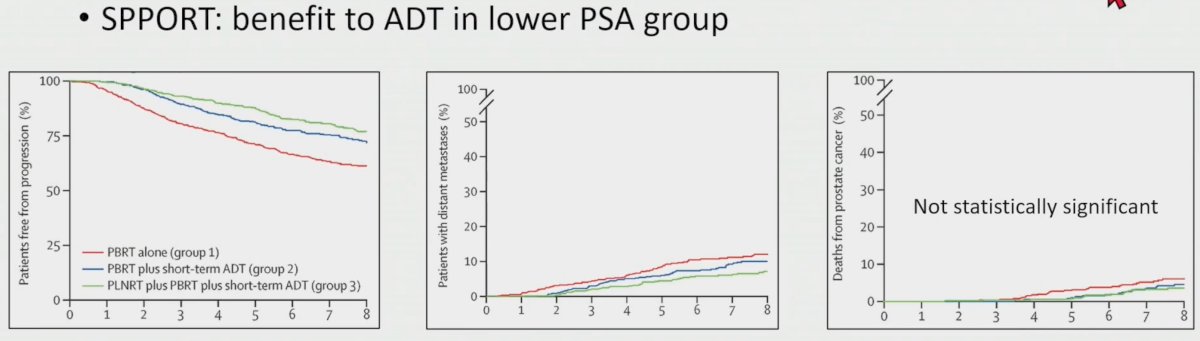
Conversely, results of the SPPORT trial support the benefit of ADT in the lower PSA group. In this trial, the addition of short-term ADT to prostate bed radiotherapy in the salvage setting (+/- pelvic nodal radiotherapy) for patients with a rising PSA of 0.1 – 2 ng/ml following a radical prostatectomy was associated with improvements in disease progression and distant metastatic outcomes, albeit with no overall survival benefit to date.
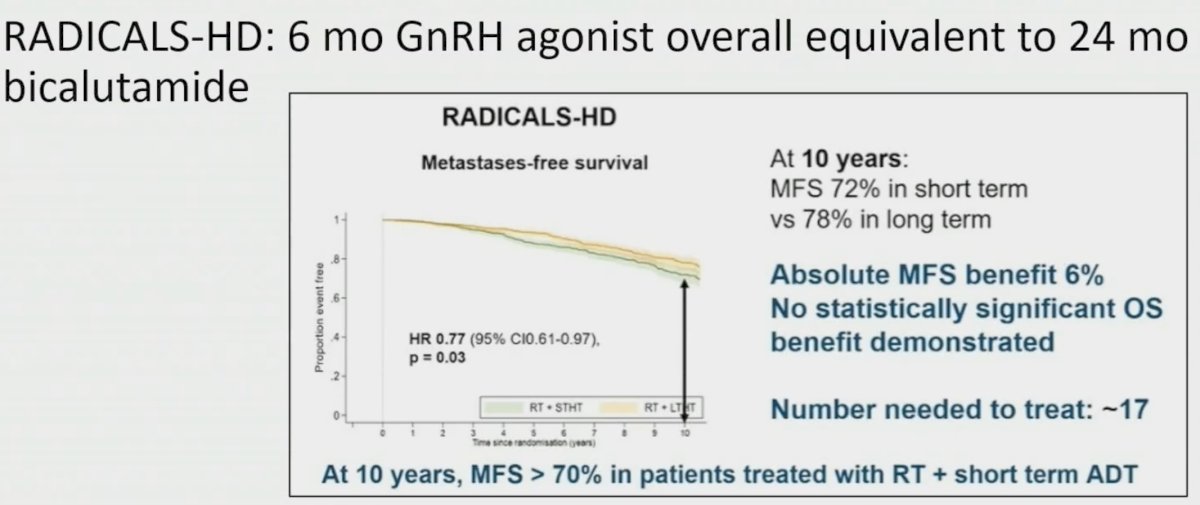
What about duration of ADT in the salvage setting? This decision may be informed by results of the RADICALS-HD trial presented at ESMO 2022. In this trial, a two-group comparison was performed between patients receiving short (6 months of GnRH agonist) versus long-term (24 months bicalutamide) ADT. At 10 years, metastasis-free survival was improved from 72% to 78% (absolute benefit of 6%). However, no statistically significant overall survival benefit was demonstrated.
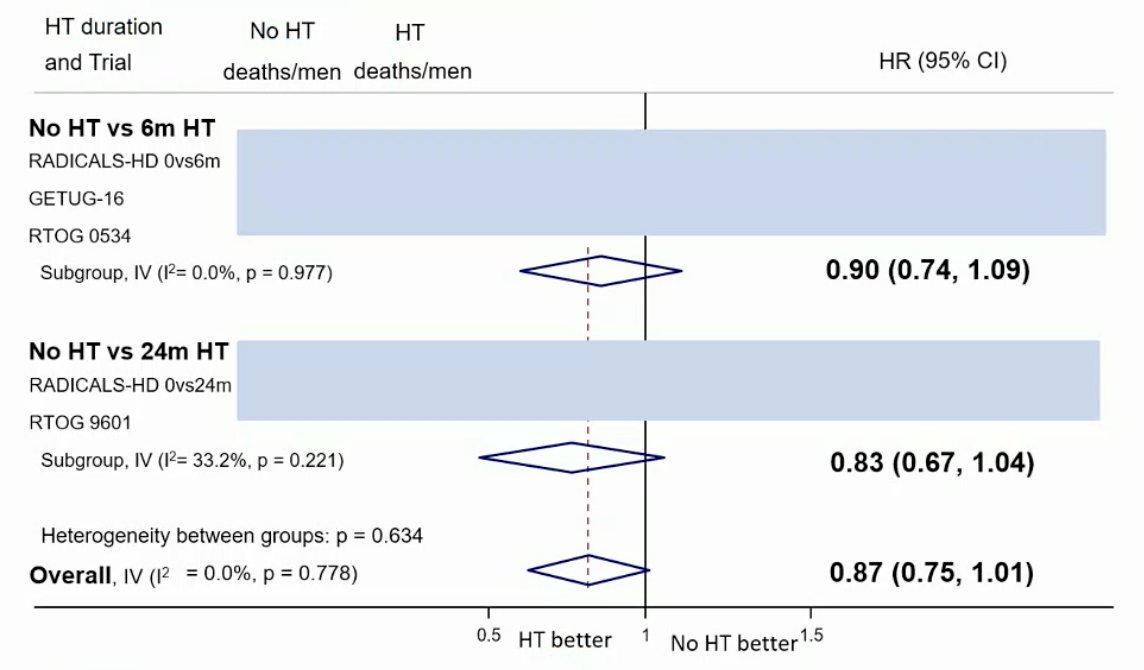
Subsequently, the DADSPORT meta-analysis collaboration conducted a systematic review and meta-analysis of results from NRG/RTOG 9601, GETUG-AFU 16, NRG/RTOG 0534, and RADICALS-HD trials to assess the effect of hormone therapy in men receiving radiotherapy following radical prostatectomy for localized prostate cancer. At a median follow-up of ≥8 years, there was no clear improvement in overall survival with hormone therapy compared to no hormone therapy (HR: 0.87, 95% CI: 0.75 – 1.01), irrespective of whether hormone therapy was 6 months or 24 months.
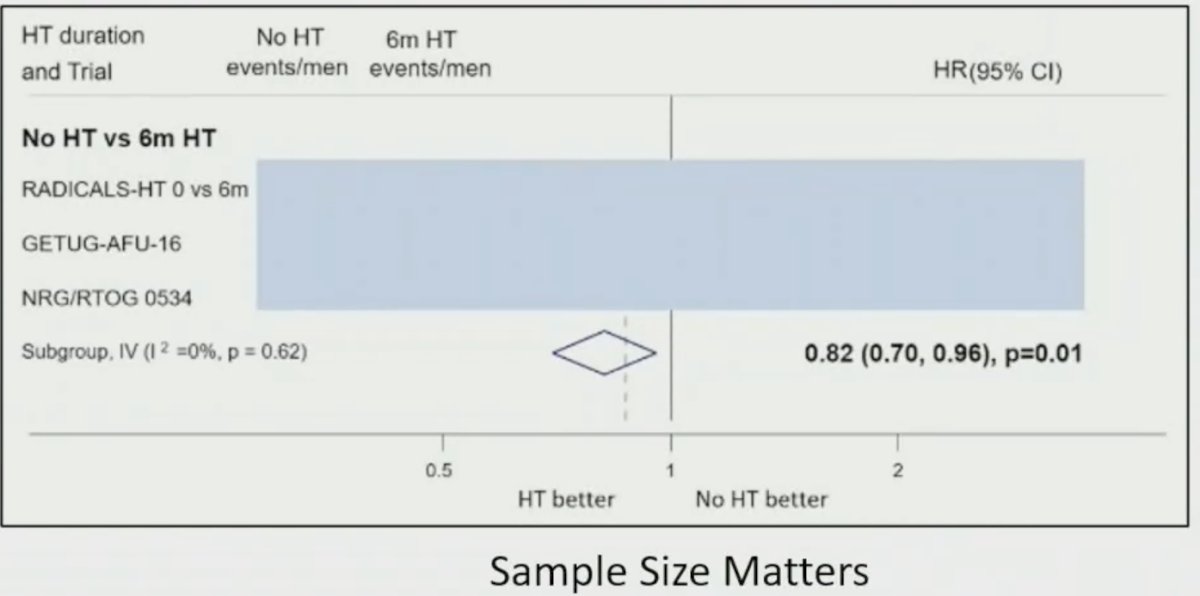
However, a subsequent analysis that only included the 3 trials that evaluated no versus short-term ADT (GETUG-AFU 16, RTOG 0534, and RADICALS-HD) demonstrated that 6 months of ADT was associated with significant improvements in overall survival, highlighting the importance of sample size and patient/trial selection in this setting.
Based on these results, Dr. Rajkumar argued that ADT in the salvage setting may be considered for a broader patient population, and not just those with a PSA >0.6 ng/ml. Other risk factors that she considers when counselling patients about concurrent ADT use in the salvage setting include:
- Gleason score: 8-10
- pT3-4 disease and/or pN1
- PSA doubling time < 10 -12 months
- Margin status
- PSA persistence
- Presence/absence of gross disease
Next, Dr. Rajkumar asked: How does 2nd generation ADT fit in the salvage setting? This is a rapidly evolving space with two phase II and 1 phase III trial recently published in this setting.
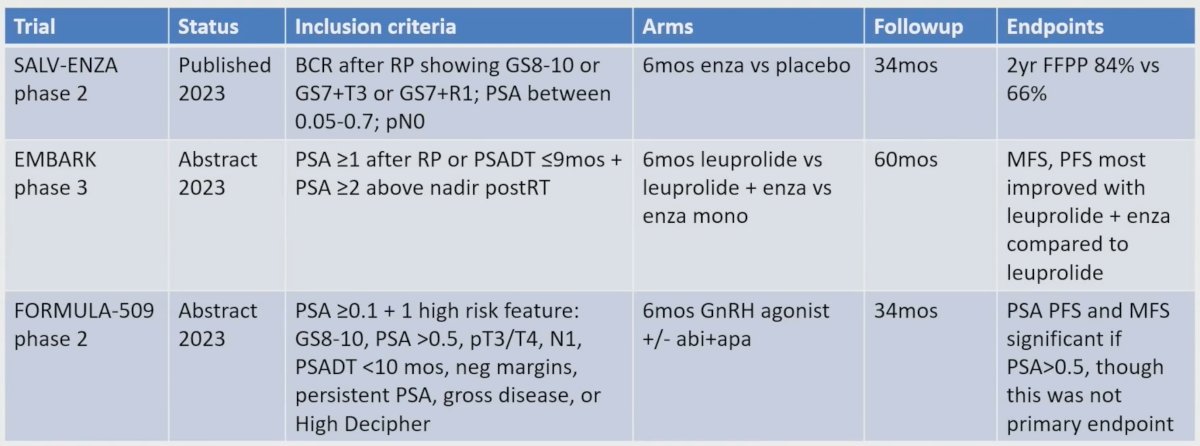
The SALV-ENZA trial randomized patients with evidence of biochemical recurrence after radical prostatectomy, PSA 0.05 – 0.7 ng/ml, and GS 8-10 or GS7 with pT3 disease or GS7 with positive margin status to 6 months of enzalutamide or placebo. At a median follow-up of 34 months, patients receiving enzalutamide had improvements in 2-year PSA progression-free survival from 66% to 84%.4
The phase III EMBARK trial was presented at AUA 2023 and included patients with PSA ≥1 ng/ml after RP or ≥2 ng/ml above nadir after primary EBRT, with a PSA doubling time of ≤9 months. At a median follow-up of 5 years, the combination of enzalutamide/leuprolide, versus leuprolide alone, demonstrated a significant improvement in MFS (HR: 0.42, 95% CI: 0.31 – 0.61, p<0.0001).
FORMULA-509 is a phase II trial that included patients with a PSA ≥0.1 ng/ml and 1 high-risk feature who received 6 months of a GnRH agonist +/- abiraterone and apalutamide. This trial failed to meet its primary endpoint but demonstrated that PSA progression-free and metastasis-free survivals were improved in patients with a PSA >0.5 ng/ml who received the additional androgen receptor pathway inhibitors.
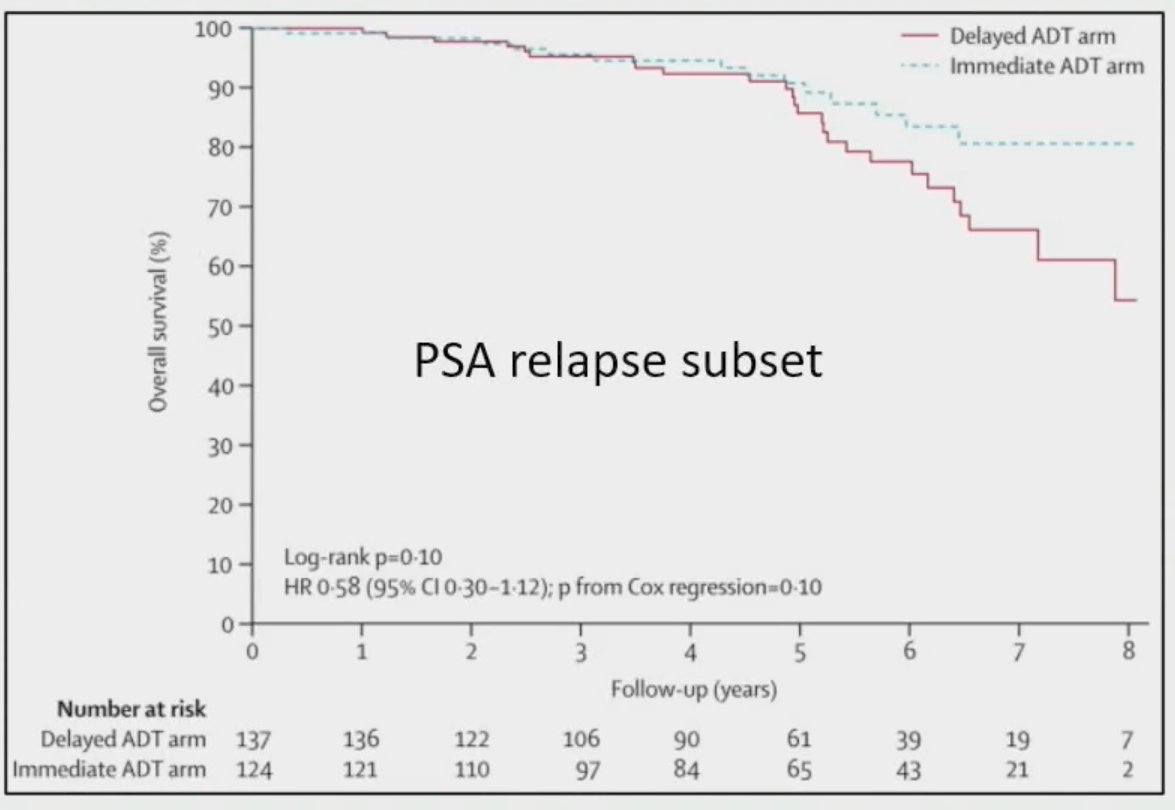
What about the treatment of patients with a rising PSA following definitive or salvage radiotherapy? As mentioned, the EMBARK trial included patients with a PSA 2 ng/ml above nadir following primary EBRT with a PSA doubling time of ≤9 months and showed that enzalutamide addition to leuprolide improves MFS. Furthermore, results of the TOAD trial demonstrated that immediate ADT, compared to delayed ADT (>2 years following randomization unless symptoms or metastases developed or PSA doubling decreased to <6 months) was associated with improvements in 5-year overall survival (91.2% versus 86.4%; HR: 0.55, 95% CI: 0.30 -1.00, p=0.05) and improved prostate cancer complication-free survival.5

However, overall, the data for use of ADT in the post-radiotherapy salvage setting remains sparce and this has been acknowledged by current guidelines:
“Intermittent ADT therapy can be offered to patients with higher-risk biochemical recurrence, with most definitions of high-risk including PSA doubling time less than 10 to 12 months, Gleason score 8 or greater, or biochemical relapse interval of up to 18 months".
Dr. Rajkumar concluded her presentation with the following take home messages:
- Consider abiraterone or other 2nd generation ADT for patients with intact disease with 2+ high-risk features or positive nodes
- ADT along with salvage RT is highly individualized, with factors like Gleason score 8-10, PSA >0.5 ng/ml, pT3/T4, pN1, PSA doubling time <10-12 months, positive margin status, PSA persistence after prostatectomy, presence of gross disease, and genomic classification helping to guide discussions
- With a negative PET, PSA doubling time is likely the strongest factor for deciding when to initiate ADT with biochemical recurrence after salvage radiotherapy, although other risk factors should be weighed as well
- Can administer ADT intermittently
- We look forward to randomized data to help guide use of ADT after SBRT
- Open field for biomarkers - extracellular vesicles, ctDNA, Tempus, more coming
1. Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022;399(10323):447-60.
2. Feng FY, Huang H, Spratt DE, et al. Validation of a 22-Gene Genomic Classifier in Patients With Recurrent Prostate Cancer: An Ancillary Study of the NRG/RTOG 9601 Randomized Clinical Trial. JAMA Oncol. 2021;7(4):544-52.
3. Pollack A, Karrison TG, Balogh A, et al. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): an international, multicentre, randomised phase 3 trial. Lancet. 2022;399(10338):1886-901.
4. Tran PT, Lowe K, Tsai H, et al. Phase II Randomized Study of Salvage Radiation Therapy Plus Enzalutamide or Placebo for High-Risk Prostate-Specific Antigen Recurrent Prostate Cancer After Radical Prostatectomy: The SALV-ENZA Trial. J Clin Oncol. 2023;41(6):1307-17.
5. Duchesne GM, Woo HH, Bassett JK, et al. Timing of androgen-deprivation therapy in patients with prostate cancer with a rising PSA (TROG 03.06 and VCOG PR 01-03 [TOAD]): a randomised, multicentre, non-blinded, phase 3 trial. Lancet Oncol. 2016;17(6):727-37.
Presented By: Dr. Anne Rajkumar, MD, Assistant Professor, Department of Radiation Oncology, Mayo Clinic, Rochester, MN
Written By: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 American Society for Therapeutic Radiation Oncology (ASTRO) 65th Annual Meeting held in San Diego, CA between October 1st and 4th, 2023