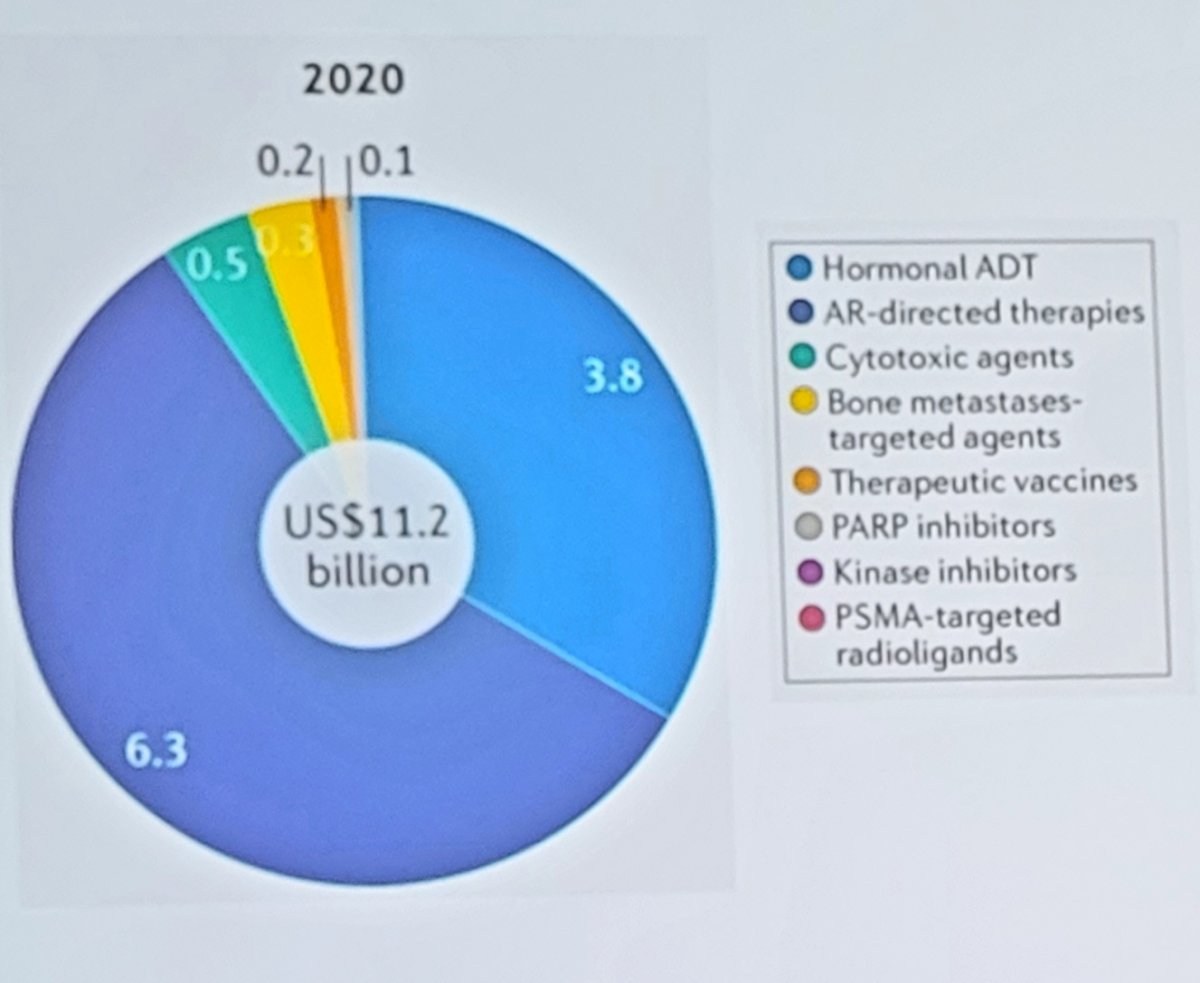
(UroToday.com) The Society of Urologic Oncology (SUO) annual winter meeting included an advanced prostate cancer session and a presentation by Dr. Michael Morris discussing the VISION trial and integration of PSMA-targeted therapy for advanced prostate cancer. Dr. Morris notes that radioligand therapy has undergone an evolution in targeting from hydroxyapatite targeting to tumor targeting. Based on 2020 data estimating the market sales ($11.2 billion) by drug class for advanced prostate cancer, there has been limited use ($0.3 billion) of bone metastases-targeted agents:
This is likely secondary to several reasons, including increased risk of fracture when Radium-223 is combined with abiraterone, and the somewhat more logistically difficult delivery of therapy compared to the AR-directed therapies.
As PSMA is highly expressed in prostate cancer and mCRPC lesions, the combination of PSMA-617 with the beta-emitter lutetium allows for the targeted delivery of ß-particle radiation to PSMA-expressing cells and the surrounding microenvironment. Within this context, the VISION trial is an international, randomized, open-label phase III study evaluating 177Lu-PSMA-617 in men with PSMA-positive mCRPC who had previously received treatment with next-generation androgen receptor signaling inhibition (abiraterone, enzalutamide, etc) and one or two prior lines of taxane chemotherapy.1 Additionally, patients must have had an ECOG performance status of 0-2 and life expectancy of at least 6 months. Importantly, patients must have had PSMA-positive disease on the basis of a central review of 68Ga-PSMA-11 staging scans. PSMA positivity was defined as uptake greater in metastatic lesions than in the liver. Further, they could have no PSMA-negative metastatic lesions.
Following enrollment, patients were randomized in a 2:1 fashion to receive either 177Lu-PSMA-617 (7.4 GBq every 6 weeks x 6 cycles) plus standard of care (SOC) or SOC alone. SOC treatments were at the discretion of the treating investigator; however, cytotoxic chemotherapy, immunotherapy, and radium-223 were explicitly excluded. Most patients received alternative androgen-directed therapies while others received palliative radiotherapy and glucocorticoids. The trial schema for VISION is as follows:

The trial assessed two alternate primary endpoints: radiographic progression-free survival (rPFS) using PCWG3 criteria by independent central review (ICR) and overall survival (OS). In addition to these two primary endpoints, they also assessed key secondary endpoints of objective response rate (ORR; RECIST v1.1), disease control rate (DCR), and time to first symptomatic skeletal event (SSE) as well as other secondary endpoints including safety and tolerability, biomarkers including PSA, and health-related quality of life and pain.
Among 1,179 screened patients, the VISION trial enrolled 831 patients between June 4, 2018 and October 23, 2019, including 551 patients were allocated to 177Lu-PSMA-617 + SOC and 280 were allocated to SOC only. Over a median study follow-up of 20.9 month, treatment with 177Lu-PSMA-617+ SOC significantly improved overall survival by a median of 4.0 months (median OS, 15.3 vs 11.3 months; HR, 0.62 [95% CI: 0.52, 0.74]; p < 0.001, one-sided), compared to SOC alone, in the overall cohort of all randomized patients (n=831). The second alternate primary endpoint showed that treatment with 177Lu-PSMA-617 + SOC significantly improved rPFS by a median 5.3 months (median rPFS, 8.7 vs 3.4 months; HR, 0.40 [99.2% CI: 0.29, 0.57]; p < 0.001, one-sided). Additionally, 177Lu-PSMA-617 + SOC significantly improved time to first symptomatic skeletal event by a median 4.7 months (median, 11.5 vs 6.8 months; HR, 0.50 [95% CI: 0.40, 0.62]; p < 0.001):

First presented at ESMO 2021 by Dr. Karim Fizazi, health-related quality of life was assessed in the pre-specified rPFS analysis set comprising 581 of the 831 randomized patients (177Lu-PSMA-617 arm, n = 385; control arm, n = 196). Health-related quality of life and pain time-to-worsening analyses favored the 177Lu-PSMA-617 arm. For the FACT-P total score, time to worsening was 9.7 months for 177Lu-PSMA-617 compared to 2.4 months for standard of care alone (HR 0.46, 95% CI 0.35-0.61):

Additionally, for the BPI-SF pain intensity score, time to worsening was 14.3 months for 177Lu-PSMA-617 compared to 2.9 months for standard of care alone (HR 0.45, 95% CI 0.33-0.60):

In addition to these endpoints, the addition of 177Lu-PSMA-617 to SOC statistically significantly improved all key secondary endpoints, including ICR-determined ORR (29.8% vs 1.7%) and ICR-determined DCR (89.0% vs 66.7%). Further, PSA responses (whether defined as a 50% decrease or an 80% decrease) were significantly more common among those treated with 177Lu-PSMA-617 + SOC. While a higher rate of high-grade (grade 3-5) treatment-emergent adverse events were expected and observed with 177Lu-PSMA-617 (28.4% vs 3.9%), overall therapy was well tolerated. In terms of specific adverse events, treatment with 177Lu-PSMA-617 + SOC was associated with increased rates of bone marrow suppression, xerostomia, and nausea and vomiting.
Currently, the prostate cancer treatment landscape is both exciting and somewhat convoluted. Further 177Lu-PSMA-617 data is expected in the coming years with the PSMA Fore and PSMA Addition trials. The PSMA Fore trial is assessing 177Lu-PSMA-617 targeted radioligand therapy earlier in the disease course, randomizing mCRPC patients with disease progression on previous AR therapy and no prior taxane chemotherapy 1:1 to 177Lu-PSMA-617 targeted radioligand therapy versus a change in AR inhibitor therapy:

The PSMA Addition trial is testing 177Lu-PSMA-617 targeted radioligand therapy even earlier in advanced prostate cancer, specifically metastatic hormone-sensitive disease (mHSPC). This trial will randomize untreated or minimally treated patients appropriate for standard of care 1:1 to standard of care + 177Lu-PSMA-617 targeted radioligand therapy or to standard of care alone:

As follows is a schematic with regards to how to potentially optimize patient selection as highlighted by Dr. Morris:

However, Dr. Morris notes that there are several considerations with regards to moving 177Lu-PSMA-617 earlier in the disease course:
- The stakes are greater for long-term toxicity
- Micrometastatic disease may be more amenable to alpha emitters
- Monotherapy versus utilization of ADT/ARSI to increase PSMA expression and maximize dosimetry
- Imaging may not be informative for patient selection
- There is a risk of overtreatment
Thus, with regards to biomarker optimization, is PSMA imaging necessary? What is the minimum amount of testing needed to deliver care to the most patients with the least number of systemic barriers? In VISION, 68Ga-PSMA-11 PET/CT was positive in ~87% of patients, thus meeting PSMA-positive mCRPC criteria for enrollment. Looking at the TheraP trial,2 which assessed 177Lu-PSMA-617 versus cabazitaxel, Dr. Morris notes that there are hints of heterogeneous biology and a potential opportunity for biomarker selection. All patients in this trial underwent both Ga-68-PSMA-PET/CT and F-18-FDG-PET/CT prior to randomization, and to be eligible for inclusion patients must have had a high avidity lesion on PSMA PET/CT (SUV max >20 at any site) with measurable disease with an SUV max of 10 or greater; there could be no sites of disease which were FDG positive but PSMA negative. By selecting patients that have PSMA/FDG PET concordance, perhaps we are able to select patients that will benefit most from 177Lu-PSMA-617 targeted radioligand therapy. Other biomarker candidates may include (i) the high-risk disease population, (ii) MMR patient population, (iii) ctDNA positive population, and (iv) circulating tumor cell PSMA expression for patients with non-imageable disease.
Dr. Morris concluded his presentation of integrating PSMA-targeted therapy for advanced prostate cancer with the following summary points:
- Radioligand therapy improves how patients feel, function, and survive
- In post-ARPI/chemotherapy patients, tumor-directed radioligand therapy achieves this trifecta, even in those with soft tissue disease
- 177Lu-PSMA-617 opens the door to a new drug class for prostate cancer, new sequencing studies, and new combinations
- The optimal “advanced” patient population has yet to be completed defined
Presented by: Michael J. Morris, MD, Prostate Cancer Section Head, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 Society of Urologic Oncology (SUO) Winter Annual Meeting, Orlando, FL, Wed, Dec 1 – Fri, Dec 3, 2021.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.