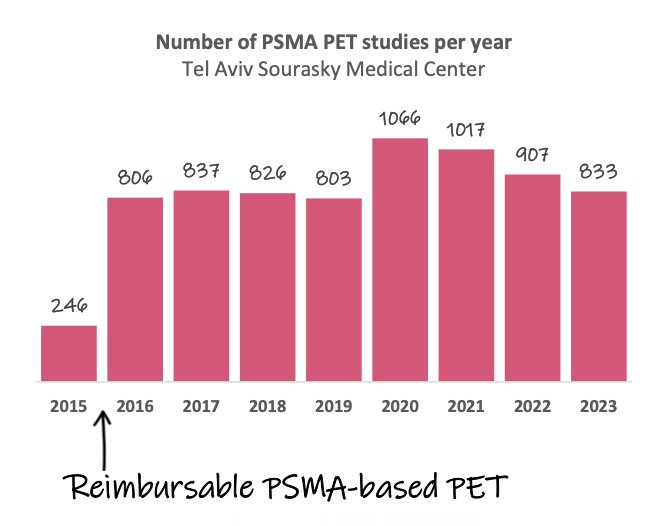
(UroToday.com) The 2024 Society of Nuclear Medicine & Molecular Imaging (SNMMI) annual meeting featured a session on prostate cancer and a presentation by Dr. Dan Cohen discussing PSMA PET and insights gained from eight years of reimbursable imaging. Dr. Cohen started his presentation by highlighting that in January 2016, PSMA-based PET imaging was added to the Israeli national list of reimbursable health services. Subsequently, Israel emerged as one of the earliest countries in the world to apply PSMA-based PET in consecutive patients:
As such, ongoing data has transformed the way prostate cancer is understood and approached clinically. For in vivo molecular imaging, signals must penetrate biological tissues and the detector must have high sensitivity. PSMA is a prostate-specific membrane antigen that is overexpressed in prostate cancer cells compared to normal prostate tissue. In the 1980s, PSMA was targeted with the 111In-Abs, which required the antibody to traverse the cellular membrane and bind to the intracellular portion of the PSMA protein, with limited signal intensity: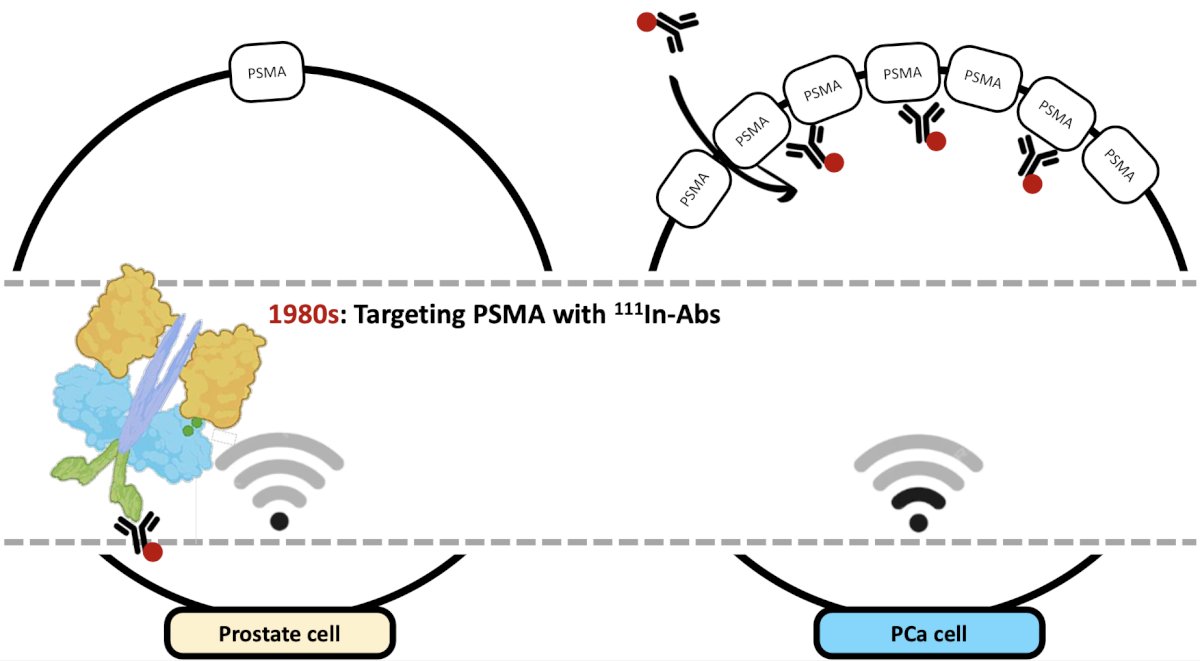
However, in the 2010s, there was development of targeting with labeled PSMA ligands, allowing targeting of the extracellular portion of the PSMA protein:
Thus, the revolution of in vivo whole-body PET imaging for prostate cancer arrived. In the management of prostate cancer, the general workflow typically includes a noninvasive assessment with a DRE (T stage) or mpMRI (providing a PI-RADS score) for men with an elevated PSA. This is followed by a definitive diagnosis with a prostate biopsy, leading to an ISUP Gleason Grade, and followed by whole-body imaging for those diagnosed with clinically significant prostate cancer. Historically, this may have included a CT and bone scan (more recently a PSMA PET/CT), leading to the development of a therapy strategy:
PSMA PET/CT may: (i) accurately identify prostate cancer lesions, (ii) stratify patients at diagnosis, and (iii) guide treatment selection, ie surgery versus radiotherapy, radiotherapy alone, or hormonal therapy. Subsequently, PSMA PET/CT may allow monitoring of response (versus stable versus progression) and provide continued follow-up. During this time, PSMA PET/CT may detect localized recurrence sites and patterns of recurrence (prostate bed recurrence, oligometastatic recurrence, and poly-metastatic recurrence). For those patients with disease progression, PSMA PET/CT may allow for assessment of molecular resistance mechanisms and monitor clinical deterioration. Dr. Cohen then discussed the following topics based on vast amounts of published data:
- The different PSMA ligands
- The utility of PSMA PET for local staging
- Revisiting previously held conceptions for metastatic staging
- From “black spots” to molecular insights
- Can PSMA PET modify traditional clinical workflows?
The following figure demonstrates the chemical structure of the different PSMA ligands, including 68Ga-PSMA-617, 68Ga-PSMA-11, and 18F-PSMA-1007: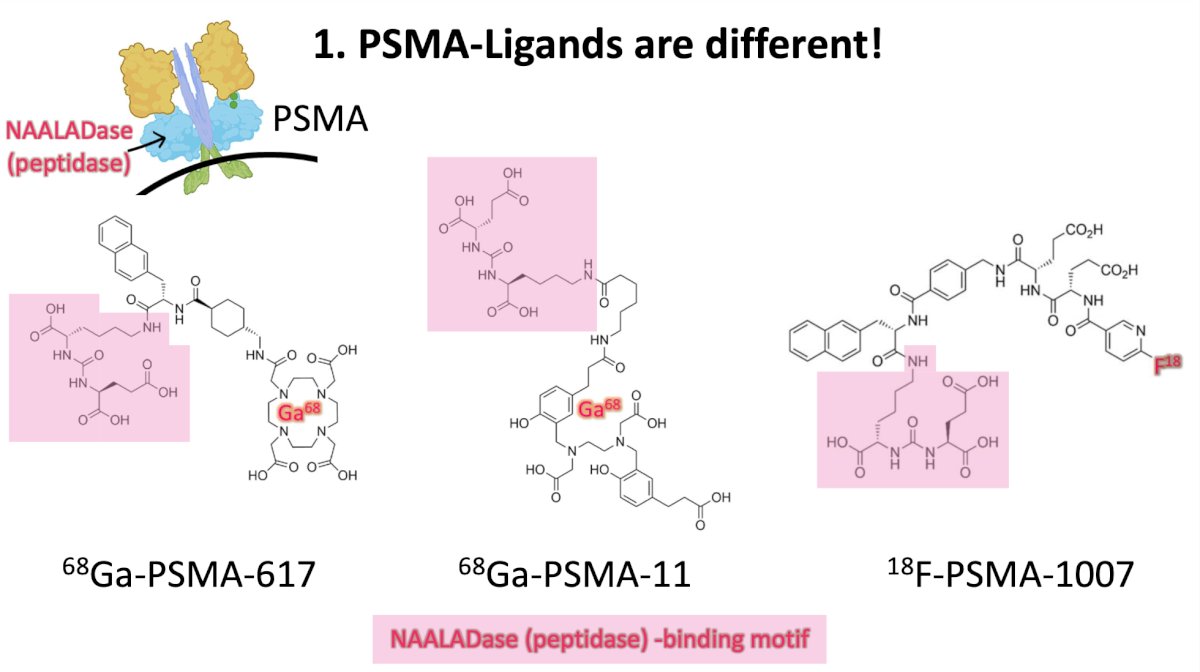
There are several other key differences between ligands, including:
- Excretion: Urinary > biliary excretion (68Ga-PSMA-11) and biliary > urinary excretion (18F-PSMA-1007)
- Half-life: t1/2 68 minutes (68Ga) and t1/2 110 minutes (18F), which leads to better spatial resolution for 18F
- Bone uptake: 18F-PSMA-1007 is associated with unspecific focal bone uptake in ~34% of scans
Dr. Cohen notes that because of more biliary excretion than urinary excretion, their departmental approach is to use 18F-PSMA-1007 in biochemical recurrence after radical prostatectomy.
With regards to local staging, how does PSMA PET/CT do for identifying extracapsular extension, seminal vesicle involvement, or involvement of nearby organs (such as lymph node involvement)? Work from Dekalo et al.1 compared PET findings and radical prostatectomy pathology specimens (n = 61) and found that 0/27 extraprostatic extension cases found at the time of radical prostatectomy were suggested by PSMA PET/CT findings. In a prospective study of 140 patients, all underwent whole-body PET-CT and subsequent pelvic PET-MRI, and there was good agreement for intra-prostatic lesions (k = 0.85), lymph node involvement (k = 0.98), and bone (k = 0.76) assessment.2 However, there was worse agreement in seminal vesicle involvement (k = 0.31) and extraprostatic extension (k = 0.25) assessment: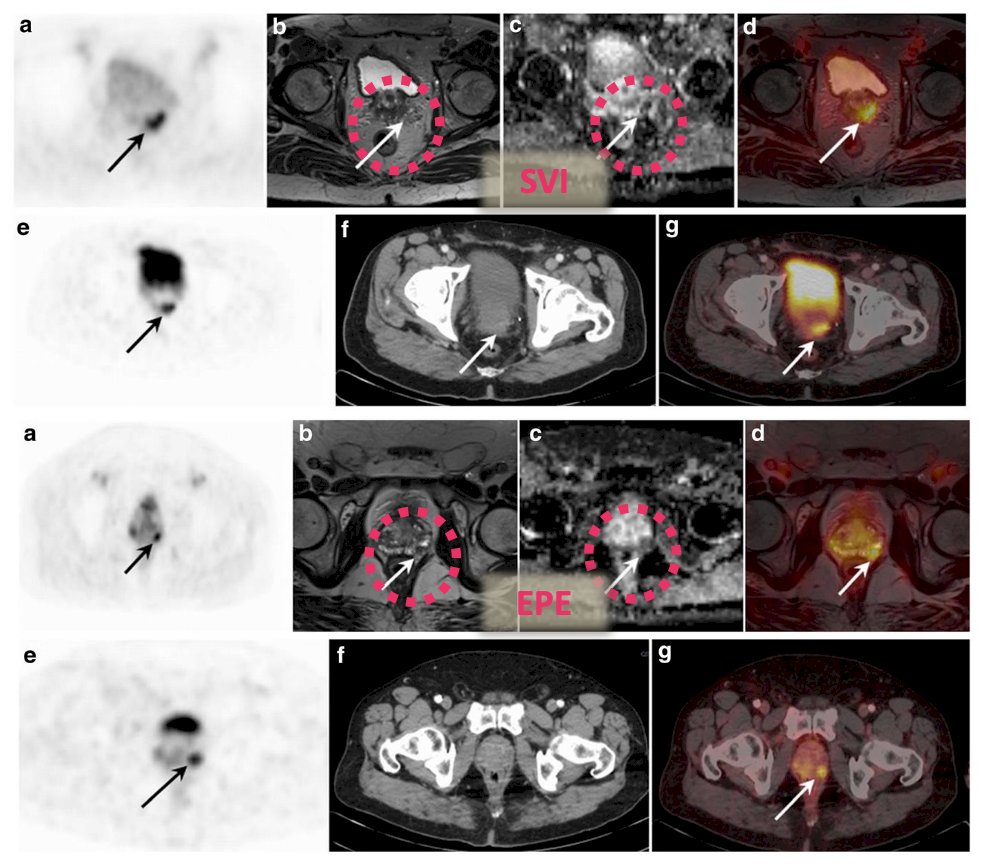
For M-staging, 99mTc-MDP bone scan mainly reported osteoblastic activity. But based on PSMA expression, are these indeed osteoblastic lesions?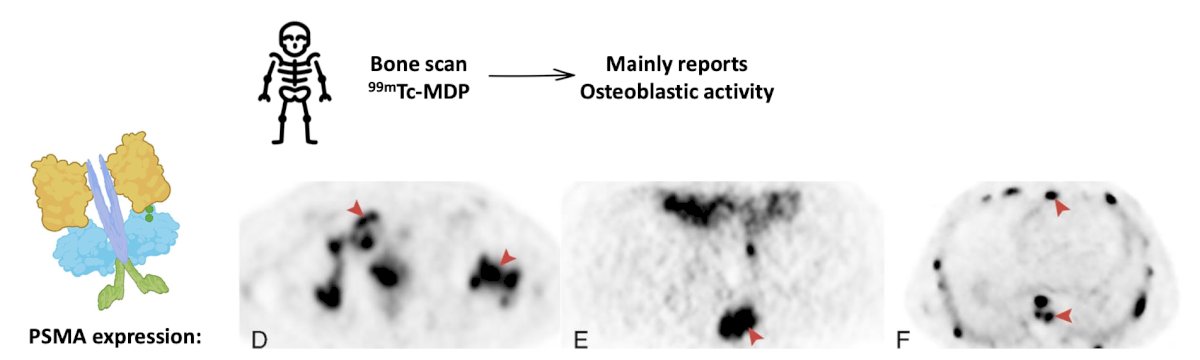
In a study by Kesler et al3 assessing the incidence and type of skeletal involvement in a large cohort of patients with newly diagnosed prostate cancer referred for Ga-68 PSMA-11 PET/CT staging, among 963 consecutive patients, bone metastases were found in 188 (19.5%). Osteoblastic type metastases were the most common type of bone metastases presented in 133 of the patients with malignant bone involvement (70.7%). Furthermore, more than half of them had only osteoblastic lesions (72 patients (38.3%)), while the other (61 patients (32.5%)) had also intramedullary and/or osteolytic type lesions: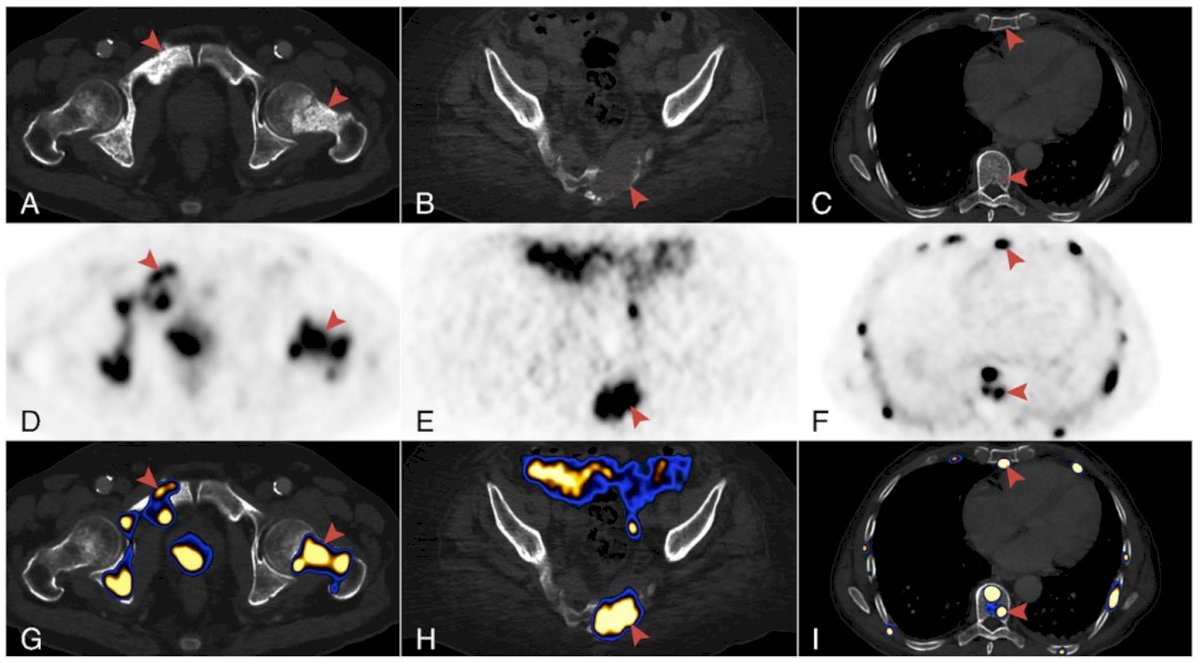
With regards to the shift from “black spots” seen on nuclear medicine bone scan to molecular insights from PSMA suggest that an increase in lesions, an increase in intensity of uptake, and the total volume of PSMA expression suggests that more equals bad disease. Additionally, even in situations where there is only a slight increase in PSA, new PSMA expression metastases indicates progressive disease:
Moreover, patients without a history of hormonal therapy may underestimate PSMA expression, where has hormone therapy may lead to PSMA expression and revealing the true burden of disease: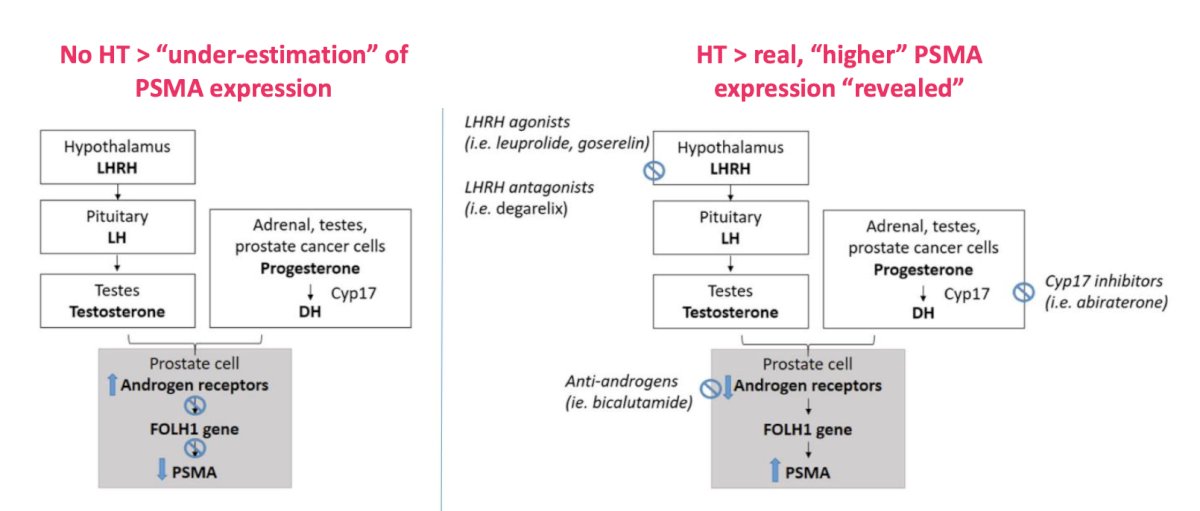
Ultimately, less expression (ie. iodine uptake, SSTR expression, or PSMA expression) is also bad. This typically represents a movement from a differentiated, castration-sensitive disease state to an undifferentiated and castration-resistant disease state: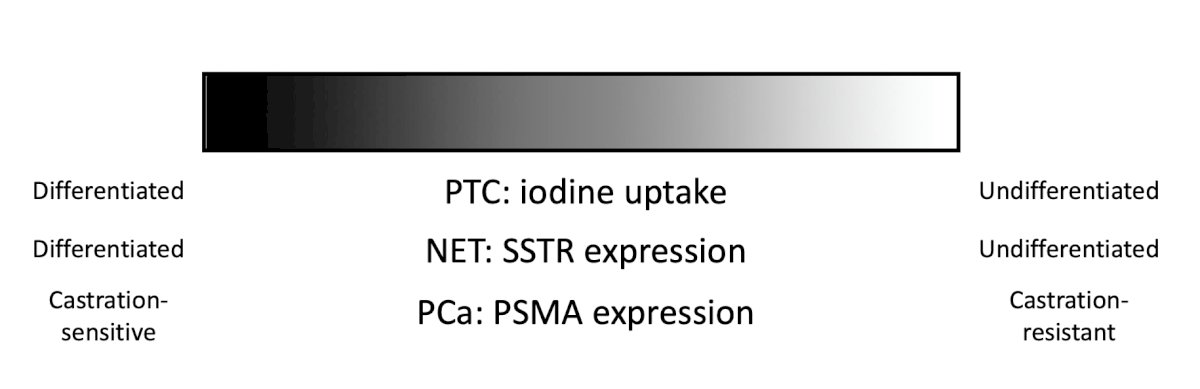
Work from Dr. Cohen’s group reviewed the available literature assessing de novo neuroendocrine differentiation versus primary prostatic neuroendocrine tumors. In cases of treatment-induced neuroendocrine differentiation, they concluded that PSMA expression may be low and that [18F]FDG or radiolabeled somatostatin-analogues should be preferred for imaging. In cases of prostatic adenocarcinoma with de novo neuroendocrine differentiation, there is superiority for radiolabeled PSMA ligands. In cases of primary neuroendocrine malignancies, the use of [18F]FDG for imaging high-grade primary prostatic neuroendocrine carcinomas and radiolabeled somatostatin-analogues for imaging well-differentiated primary prostatic neuroendocrine tumors is recommended. The aforementioned is highlighted by the following case summary:![In cases of primary neuroendocrine malignancies, the use of [18F]FDG for imaging high-grade primary prostatic neuroendocrine carcinomas and radiolabeled somatostatin-analogues for imaging well-differentiated primary prostatic neuroendocrine tumors is recommended](/images/com-doc-importer/169-snmmi-2024/snmmi-2024-psma-pet-in-patients-with-prostate-cancer-gained-insights-from-eight-years-of-reimbursable-imaging/image-11.jpg)
Finally, can PSMA PET modify traditional clinical workflows? More specifically can non-invasive assessment skip the step of definitive diagnosis (ie. biopsy) and go straight to whole-body PSMA PET/CT staging? Dr. Cohen and Kesler et al.5 assessed 100 consecutive patients > 80 years of age who underwent 68Ga-PSMA-11 PET/CT. Overall, 34 (34%) had no pre-imaging biopsy and compared to those with a prostate biopsy, those without a prostate biopsy were older (median age, 87 versus 82 years; p < 0.01), with worse performance status (p < 0.01) and higher PSA levels (median, 57 versus 15.4 ng/mL; p < 0.01). On 68Ga-PSMA-11 PET/CT, all patients that did not have a biopsy had avid disease, with trends toward higher rates of bone metastases (47.1% versus 28.8%) and overall advanced disease (50% versus 33.3%) than in those who had a biopsy. Among 39 patients with advanced disease, 38 received hormonal therapy irrespective of their biopsy status. Among those patients not undergoing a prostate biopsy with advanced disease who were referred for hormonal therapy, 12 of 13 with follow-up data showed a biochemical or imaging-based response. Dr. Cohen’s group provided the following adjusted staging algorithm suggested for elderly patients: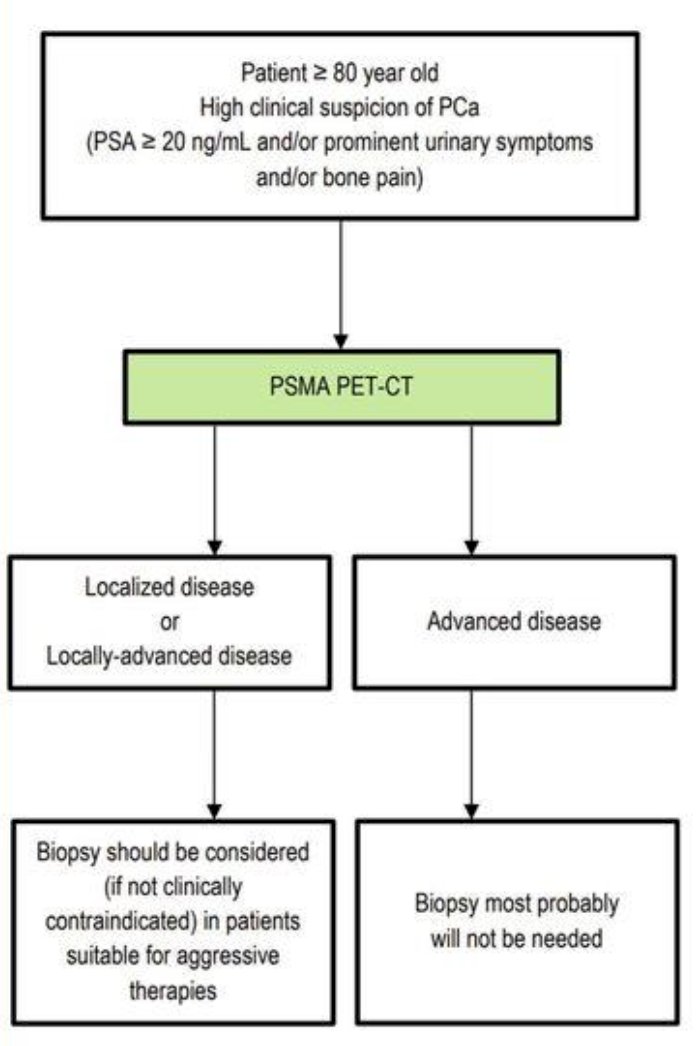
Dr. Cohen concluded his presentation discussing PSMA PET and insights gained from eight years of reimbursable imaging with the following take-home messages:
- Prostate cancer cells overexpress the PSMA glycoprotein
- Different radiolabeled PSMA ligands are available for PET:
- Report on “lesion with PSMA overexpression” or “lesion with PSMA-ligand uptake”
- Do not report on “PSMA uptake in the prostate” – this is simply wrong
- Know which PSMA ligand you use:
- There are different pharmacokinetics
- There are some different patterns of uptake
- Know what we can and cannot accurately report in local prostate cancer staging
- PSMA-based PET/CT is unlikely to predict extracapsular extension
- PSMA-positive bone metastasis exhibits different bone behavior
- Is there a decrease in PSMA expression over time? Keep in mind the possibility of dedifferentiation
- Ongoing data may further change traditional clinical algorithms
Presented by: Professor Dan Cohen, PhD, Tel-Aviv Sourasky Medical Center, Tel Aviv, Israel
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 Society of Nuclear Medicine & Molecular Imaging (SNMMI) Annual Meeting, Toronto, Ontario, Canada, Sat, June 8 – Tues, June 11, 2024.
References:
- Dekalo S, Kuten J, Mabjeesh NJ, et al. 68Ga-PSMA PET/CT: Does it predict adverse pathology findings at radical prostatectomy? Urol Oncol. 2019 Sep;37(9):574.e19-574.e24.
- Domachevsky L, Bernstine H, Goldberg N, et al. Comparison between pelvic PSMA-PET/MR and whole-body PSMA-PET/CT for the initial evaluation of prostate cancer: A proof of concept study. Eur Radiol. 2020 Jan;30(1):328-336.
- Kesler M, Kerzhner K, Druckmann I, et al. Staging 68Ga-PSMA PET/CT in 963 consecutive patients with newly diagnosed prostate cancer: Incidence and characterization of skeletal involvement. Eur J Nucl Med Mol Imaging. 2022 May;49(6):2077-2085.
- Cohen D, Krauthammer SH, Fahoum I, et al. PET radiotracers for whole-body in vivo molecular imaging of prostatic neuroendocrine malignancies. Eur Radiol. 2023 Sep;33(9):6502-6512.
- Kesler M, Cohen D, Levine C, et al. Staging prostate cancer with 68Ga-PSMA-11 PET/CT in the elderly: Is preimaging biopsy imperative? J Nucl Med. 2023 Jul;64(7):1030-1035.