(UroToday.com) The 2024 ASTRO annual meeting included a session on optimizing the therapeutic ratio in prostate cancer, featuring a presentation by Dr. William Hall discussing dose-escalated pelvic lymph node Intensity-Modulated Radiation Therapy (IMRT) with a simultaneous hypofractionated boost to the prostate for NCCN very-high-risk prostate cancer.
The treatment of pelvic lymph nodes in high-risk adenocarcinoma of the prostate is a common standard of care. However, there remains limited data as to the efficacy of higher doses of elective radiation therapy to the pelvic lymph nodes for men with very high-risk, non-metastatic adenocarcinoma of the prostate. Dr. Hall and colleagues conducted a prospective phase II study to evaluate the toxicity and efficacy of external beam dose escalation to the pelvic lymph nodes using a simultaneous integrated boost to the prostate. They also report the long-term clinical outcomes of this prospective phase II clinical trial (NCT02177292) with a median follow-up of over 10 years.
Patients were eligible for this trial if they had biopsy-proven adenocarcinoma of the prostate, a probability of lymph node risk of at least 25%, Karnofsky Performance Scale of at least 70, and no evidence of M1 disease. Pelvic lymph nodes were treated to a dose of 56 Gy over 28 fractions with a simultaneous integrated boost to the prostate to a total dose of 70 Gy over 28 fractions using IMRT: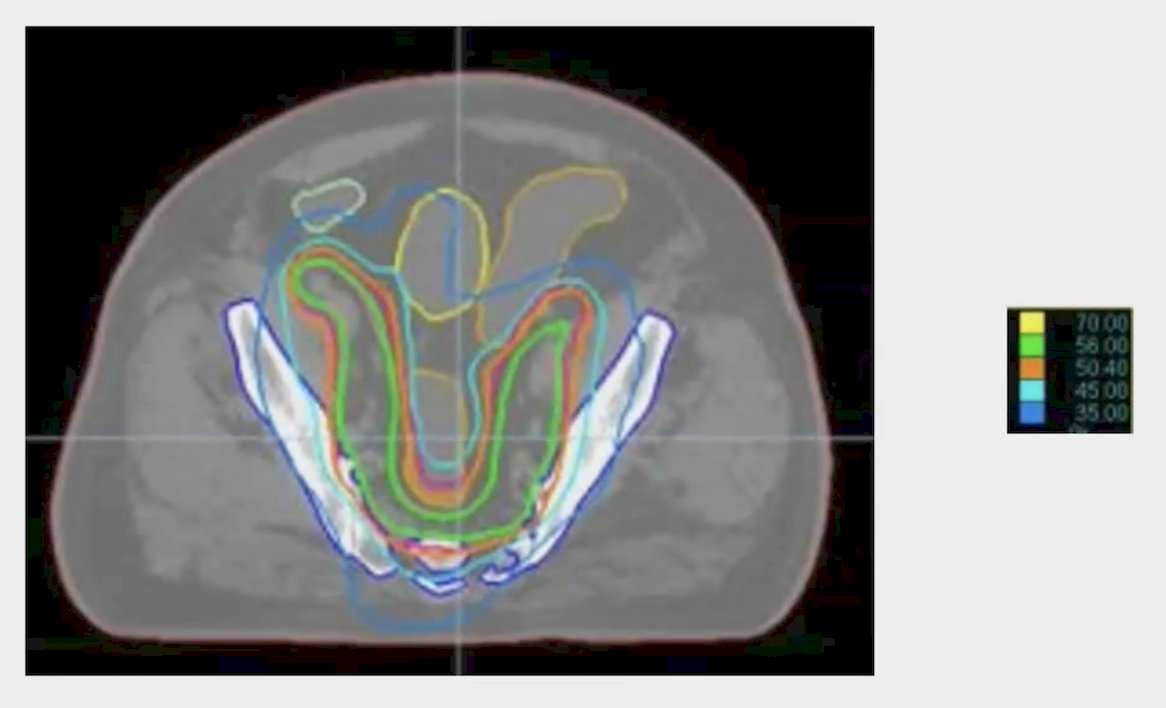
Patients were followed every three months for the first two years, every 6 months from years three to five, and annually. All patients received neoadjuvant, concurrent, and adjuvant ADT for a median of 24 months. Importantly, secondary to the time frame of the study accrual, PSMA PET/CT was not available.
There were 80 patients prospectively enrolled with 78 patients deemed eligible after final review. The mean patient age at biopsy was 72 (SD 57-86) years of age, mean pre-treatment PSA was 19.01 (SD 2.6-111.5) ng/mL, median T stage was T2c (range: T1c-T3b), 69.2% (54/78) patients had a Gleason score of 9, 28% had a Gleason score of 8, and 84% of patients were classified as NCCN very high risk. Acute and late toxicity were prospectively collected at each follow-up using CTCAE version 4.0. At a median follow up of 10.6 years, biochemical control was achieved in 92.5% of patients and distant metastasis-free survival was 96.2%. Grade 2 urinary frequency was the most common event (n = 31 patients), and grade 2 proctitis occurred in 11 patients. There were 2 patients (2.5%) that had grade 3 diarrhea, 10 patients (12.5%) had grade 3 lymphocyte depletion, but the vast majority of late toxicities were not attributed to radiation therapy.
Dr. Hall concluded his presentation discussing dose escalated pelvic lymph node IMRT with a simultaneous hypofractionated boost to the prostate for NCCN very-high-risk prostate cancer with the following take-home points:
- Nodal radiation therapy dose escalation in a modern prospective cohort of NCCN very high-risk prostate cancer resulted in extremely promising 10-year clinical outcomes
- Such results may improve even further in an era with PSMA PET-based staging
- Radiation dose intensification to the pelvic nodes warrants further study and consideration for further study in prospective randomized trials.
Presented by: William Hall, MD, Radiologist, Medical College of Wisconsin, Milwaukee, WI
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society for Radiation Oncology (ASTRO) Annual Meeting, Washington, DC, Sun, Sept 29 – Wed, Oct 2, 2024.