(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) annual meeting featured a session on applications of artificial intelligence in prostate cancer care, and a presentation by Dr. Irbaz B. Riaz discussing the use of artificial intelligence to optimize systemic therapy for prostate cancer. Dr. Bin Riaz started by highlighting the following definitions:
- Artificial Intelligence: Refers to computers or algorithms that mimic human intelligence to make data-driven decisions
- Machine learning: Is a subset of artificial intelligence that focuses on algorithms that teach itself on how to make decisions without explicit programming
- Deep learning: Is a subfield of machine learning that involves neural networks to learn and make intelligent decisions. These algorithms attempt to stimulate the human brain’s architecture and try to learn and represent complex patterns from the data
- Generative artificial intelligence: Is a subset of deep learning that has the ability to generate new content whether it be images, text, music, or other types of data. It produces content that is often indistinguishable from human-created content
The process of treatment selection for localized prostate cancer includes information gathering, risk stratification, and then finally treatment: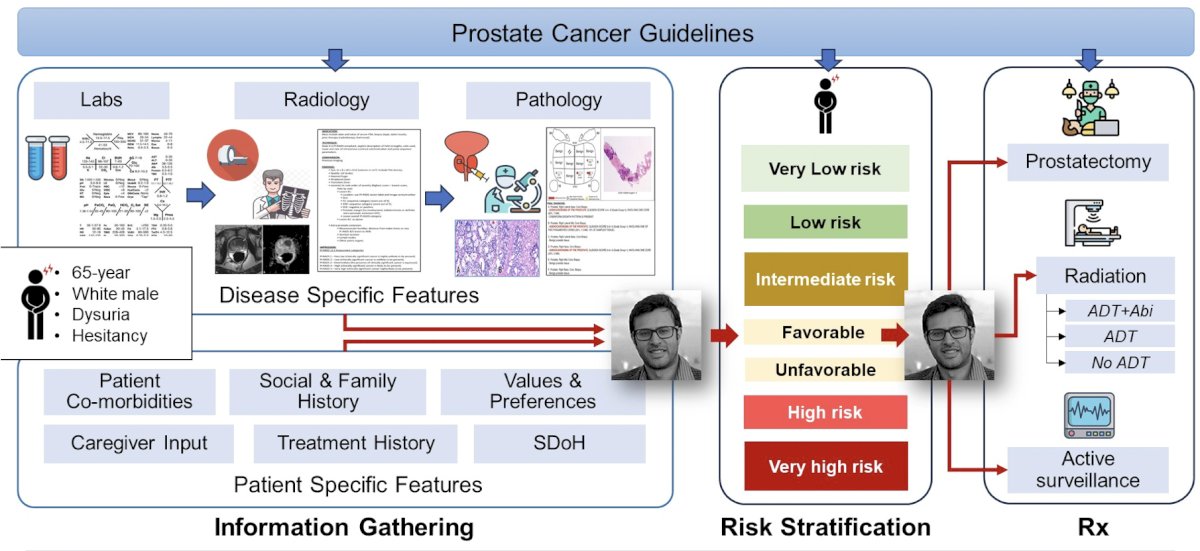
There are certainly challenges in systemic treatment selection, including:
#1 Too much to do (radiology, pathology, patient-specific features, comorbidities, patient values and preferences, labs, and guidelines)
#2: Rapidly changing evidence
#3: No real biomarkers
#4: RCTs reporting average results
For challenge #1 “Too much to do” – artificial intelligence agents may be able to act as assistants to healthcare providers. As follows is one example of how this workflow could be operationalized: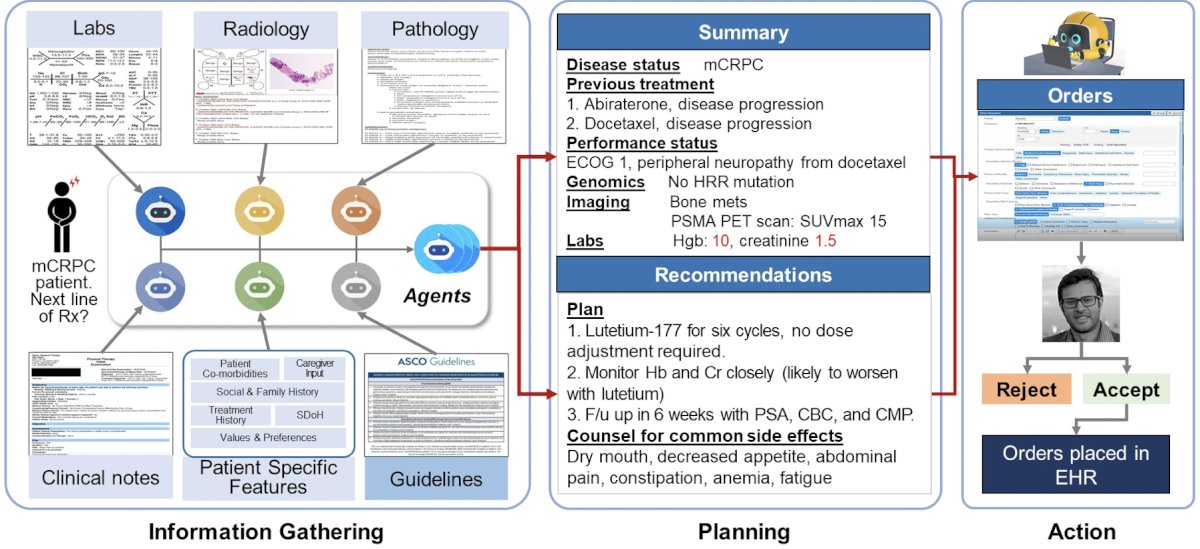
For challenge #2 “Rapidly changing evidence”, artificial intelligence may be able to create a living clinical practice guideline. Such as optimization of the standard guideline process, allowing it to update based on individual recommendations as soon as new relevant evidence becomes available. A living evidence synthesis workflow may look something like the following: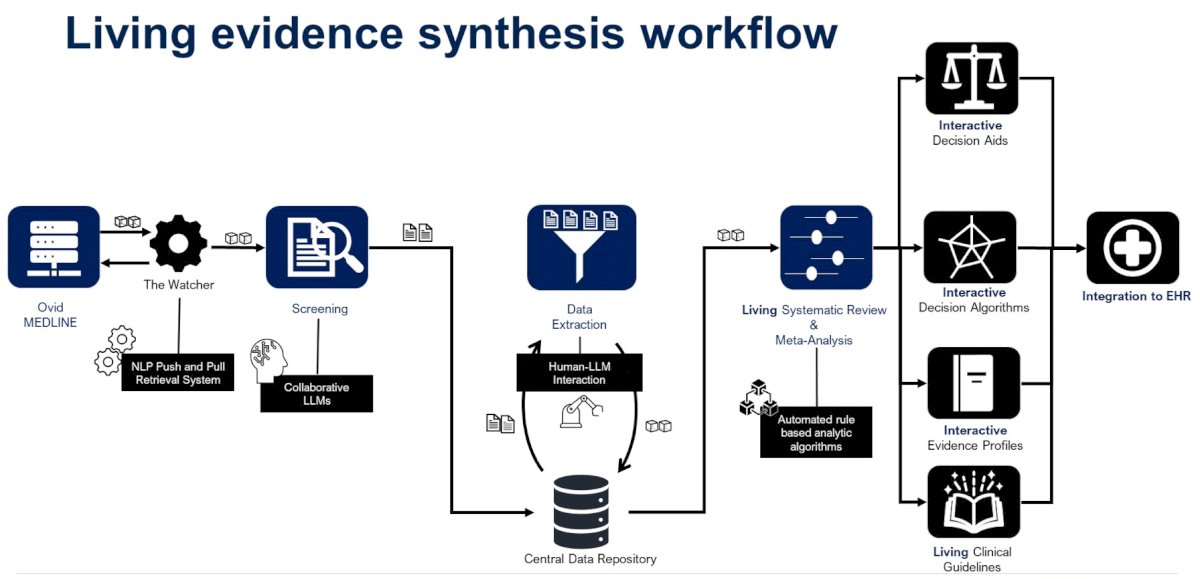
This could be used for integrating new treatment options for metastatic hormone-sensitive prostate cancer, for example:
For challenge #3 “No Real Biomarkers” this could be an opportunity for multi-modal integration, for which the conceptual framework is highlighted: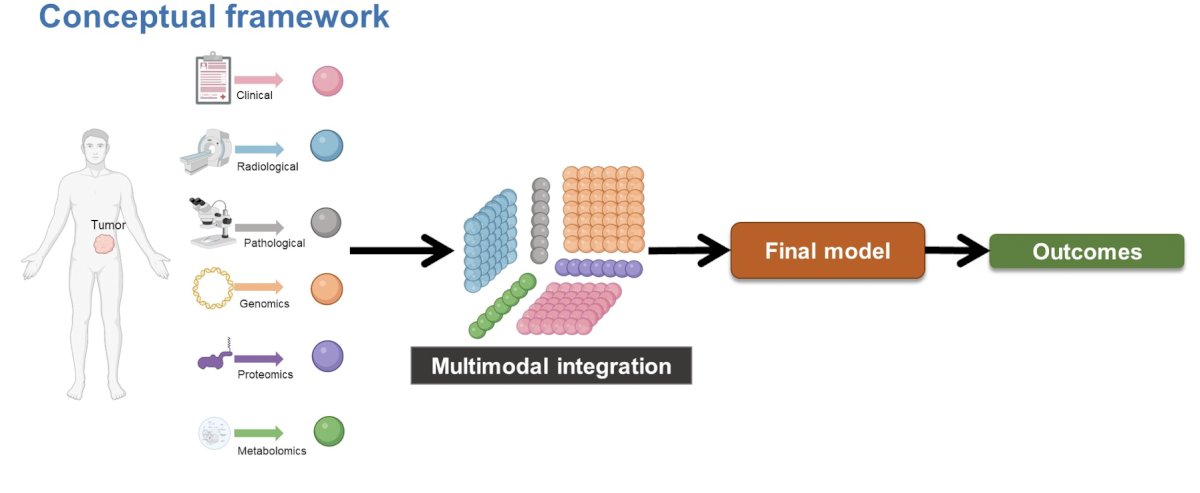
Dr. Spratt and colleagues demonstrated that a digital pathology-derived AI biomarker, the ArteraAI Prostate Test, may be used to predict short-term ADT benefits for intermediate-risk patients.1 Intermediate-risk patients who were biomarker negative did not benefit from short-term ADT (HR 1.00, 95% CI 0.63-1.56). Conversely, those with a positive biomarker status had significantly decreased distant metastases rates when short-term ADT was added to radiotherapy (HR 0.33, 95% CI 0.19-0.57):

For challenge #4 “RCTs Reporting Average Results” is a prime opportunity for artificial intelligence to individualized treatment effects via causal inference artificial intelligence: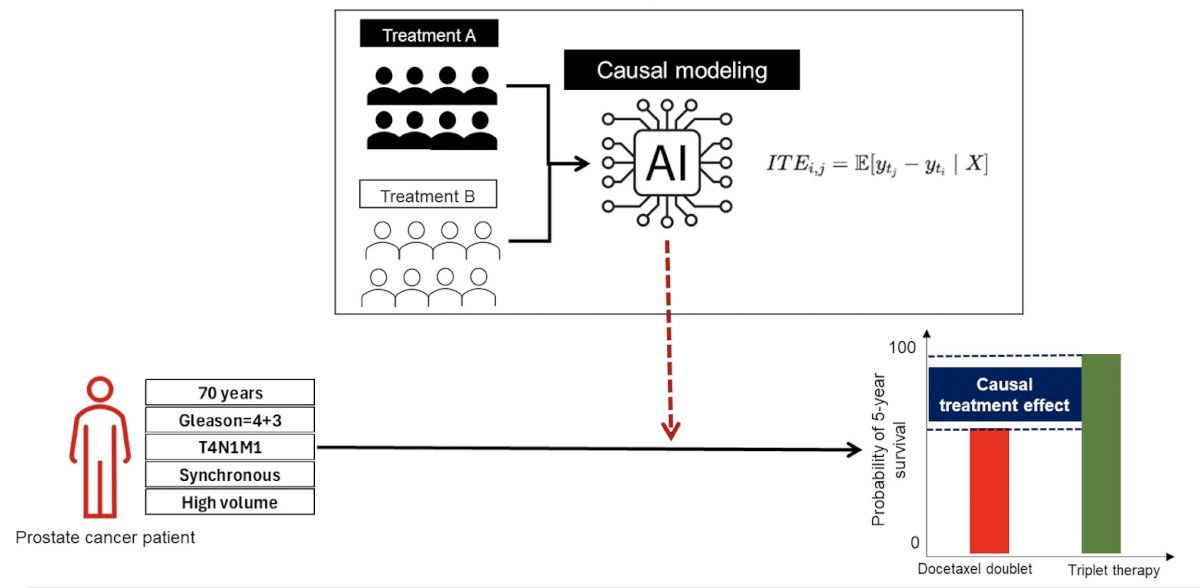
The goal here is to develop a multi-modal artificial intelligence model that integrates longitudinal data (clinical, pathological, imaging, genomic data) and then provides patient-specific treatment effects using a probabilistic deep-learning causal inference framework for prostate cancer patients.
Dr. Riaz concluded his presentation discussing the use of artificial intelligence to optimize systemic therapy for prostate cancer with the following take-home messages:
- Artificial intelligence can synthesize information for optimal systemic treatment decisions:
- Artificial intelligence agents are well poised to act as assistants to providers
- Artificial intelligence-enabled living clinical practice guidelines are feasible
- Artificial intelligence can provide novel insights from multi-modal patient data:
- Digital biomarkers utilizing multi-modal data are rapidly evolving
- Patient-specific (individualized) treatment effects is an important research topic
Presented by: Irbaz B. Riaz, MD, MBBS, Hematologist Oncology Specialist, Mayo Clinic, Phoenix, Arizona
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, May 31 – Tues, June 4, 2024.
References: