He began with an introduction to the concept of metachronous oligorecurrent prostate cancer. Such patients present with a small number of metastatic sites at least six months following initial diagnosis and treatment.
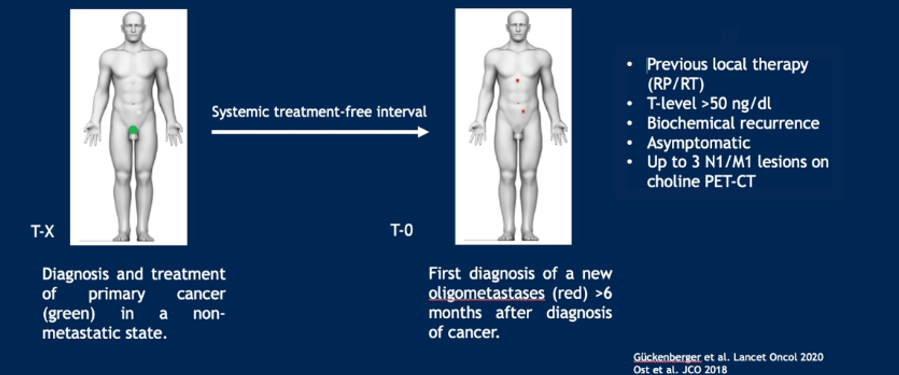
In patients fitting these criteria, he began by highlighting the historical context. In 2012, patients with symptomatic metastatic prostate cancer would be offered androgen-deprivation therapy (ADT) with asymptomatic patients either undergoing immediate or deferred ADT.
In patients undergoing a delayed ADT approach, the concept of metastasis directed therapy is typically aimed at increasing ADT-free survival. However, data from the STOMP trial has failed to demonstrate an improvement in castration-resistant prostate cancer (CRPC)-free survival thus far.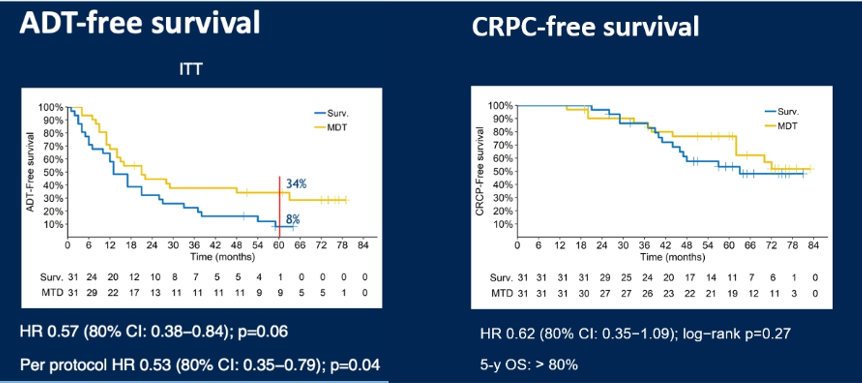
The ORIOLE trial used SABR vs. observation in terms of progression-free survival. Perhaps more importantly, the authors found that the tumor mutation burden was predictive of response to SABR with a significant benefit among those without high-risk mutations and no benefit in those with such mutations.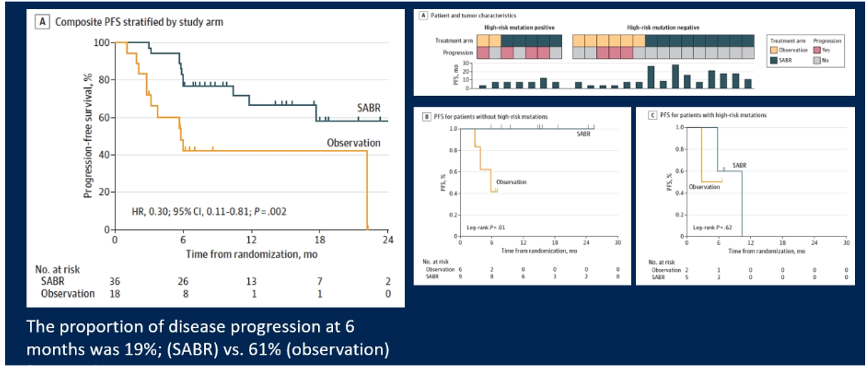
While not prostate cancer-specific, the SABR-COMET trial which randomized patients to a standard of care (SOC) vs. SOC plus SABR. This was the first trial to demonstrate an overall survival benefit to the use of SABR, in spite of no difference in time to new metastasis. Thus suggests that most patients with oligometastases have a burden of undetectable micrometastasis.
Assessing both STOMP and COMET, Dr. Ost highlighted that quality of life was not significantly affected by the use of SBRT. This can be interpreted as either proof of the safety of such an approach or proof that it fails to provide symptomatic benefit. In COMET, grade 2 or greater adverse events were much more common and grade 5 events were noted.
In conclusion, he highlighted that metastasis-directed therapy (MDT) with SBRT should not be considered standard of care until Phase III results are presented.
Presented by: Piet Ost, MD, PhD, Department of Radiotherapy and Experimental Cancer Research, Ghent University, Ghent, Belgium
Written by: Christopher J.D. Wallis, MD, PhD, Urologic Oncology Fellow, Vanderbilt University Medical Center, Twitter: @WallisCJD at the Virtual 2020 EAU Annual Meeting #EAU20, July 17-19, 2020