Introduction
Over the past decade, there have been significant advances in defining the genomic landscape of prostate cancer. The landmark study by Pritchard et al. published in The New England Journal of Medicine in 2016 demonstrated that germline DNA-repair gene mutations were present in approximately 12% of metastatic prostate cancer patients, most commonly BRCA2 (5.3%), CHEK2 (1.9%), and ATM (1.6%). Significantly, the frequency of such mutations increases across the prostate cancer spectrum – 2% in patients with NCCN localized low-to-intermediate risk tumors, 6% in those with localized high-risk tumors, and as high as 24% in patients with metastatic castrate-resistant prostate cancer (mCRPC).1 This is of utmost clinical importance as such mutations, both inherited and acquired (i.e., somatic), represent actionable clinical targets for drug therapy.
Poly (adenosine diphosphate-ribose) polymerase (PARP) inhibitors are drugs that prevent the repair of DNA single-stranded breaks and promote their conversion to double-stranded breaks leading to a synthetic lethality. These agents are most effective in homologous recombination repair (HRR)-deficient tumors (e.g., BRCA1/2), due to their compromised ability to repair DNA double strand breaks.2 In addition to breast and ovarian malignancies, PARP inhibitors have gained regulatory approval for the treatment of mCRPC patients:
- Rucaparib for BRCA1/2-mutated patients (FDA approved in 2020)3
- Olaparib for HRR-mutated patients (FDA approved in 2020)4
- Olaparib plus abiraterone for BRCA1/2-mutated patients (FDA approved in 2023)5
- Niraparib plus abiraterone for BRCA1/2-mutated patients (FDA approved in 2023)6
- Talazoparib plus enzalutamide for HRR-mutated patients (FDA approved in 2023)7
In this Center of Excellence article, we will provide an in-depth overview of the current evidence for PARP inhibitor monotherapy in prostate cancer, summarizing efficacy results from major trials and discussing the adverse event profile of these agents.
Current Evidence for PARP Inhibitor Monotherapy
Olaparib
TOPARP-A was a pivotal phase II trial of olaparib in mCRPC in which 50 patients were treated with olaparib 400 mg twice daily until disease progression.8 The primary endpoint was the composite response rate defined either as an objective response according to Response Evaluation Criteria in Solid Tumors (RECIST) criteria, or a ≥ 50% reduction in prostate-specific antigen (PSA50), or a reduction in the circulating tumor-cell count from ≥ 5 per 7.5 ml of blood to < 5 per 7.5 ml. All patients had prior treatment with docetaxel and 49 (98%) with abiraterone or enzalutamide. Sixteen of 49 (33%) evaluable patients had a response. Overall, 14 of the 16 responders had homozygous deletions, deleterious mutations, or both in DNA-repair genes — including BRCA1/2, ATM, Fanconi’s anemia genes, and CHEK2.
This was followed by TOPARP-B, an open-label, phase II trial in which men with HRR-mutated mCRPC that had progressed on ≥1 taxane therapy were treated with olaparib 400 mg or 300 mg twice daily in a randomized fashion.9 The primary endpoint was identical to the TOPARP-A trial. A targetable HRR gene aberration was found in 161 of 592 (27.2%) patients who underwent a targeted next-generation tumor sequencing. However, sequencing could not be performed on 119 (17%) of consented patients because of insufficient or poor-quality tissue. The confirmed composite response rate was 54.3% in the 400 mg cohort and 39.1% in the 300 mg cohort (p=0.14). Median radiographic progression-free survival (rPFS) was 5.5 months (95% CI: 4.4 – 8.3) in the 400 mg cohort and 5.6 months (3.7 – 7.7) in the 300 mg cohort. The predefined criteria for success were met for the 400 mg regimen but not for the 300 mg regimen.
These promising results served as the ‘precursor’ for PROfound, a randomized, open-label, phase III trial of olaparib 300 mg twice daily versus physician’s choice of standard of care therapy in men with HRR-mutated mCRPC who had disease progression while receiving a novel hormonal agent (e.g., enzalutamide or abiraterone). Patients were assigned to one of two cohorts based on their HRR gene alteration. Cohort A included patients with BRCA1, BRCA2, or ATM alterations, irrespective of co-occurring alterations in any other HRR genes. Cohort B had patients with alterations in any of the other 12 HRR genes (BRIP1, BARD1, CDK12, CHEK 1/2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D, RAD54L). Patients within each cohort were randomized in 2:1 fashion to olaparib versus standard of care . The primary endpoint was the rPFS in cohort A.
Of the 4,425 enrolled patients, 4,047 had tumor tissue available for testing and only 2,792 (69%) were successfully sequenced. A qualifying alteration in one or more of the 15 HRR genes was detected in 778 of 2,792 patients (28%). Median rPFS was significantly longer in the olaparib group than in the standard of care group (7.4 months versus 3.6 months; HR: 0.34; 95% CI: 0.25 – 0.47; p<0.001).
The confirmed objective response rate (ORR) was 33% in the olaparib group and 2% in the standard of care group (odds ratio 20.9; 95% CI: 4.2 – 379.2; p<0.001). The median time to pain progression was also significantly longer in the olaparib group (HR: 0.44; 95% CI: 0.22 – 0.91; p=0.02). The final overall survival (OS) analysis demonstrated that olaparib improved OS in cohort A from a median of 14.7 to 19.1 months (HR: 0.69, 95% CI: 0.50 – 0.97). Notably, 84% of patients with imaging-based disease progression had crossed over from the standard of care arm to olaparib at the time of analysis, which highlights the efficacy of earlier use of olaparib in this setting.10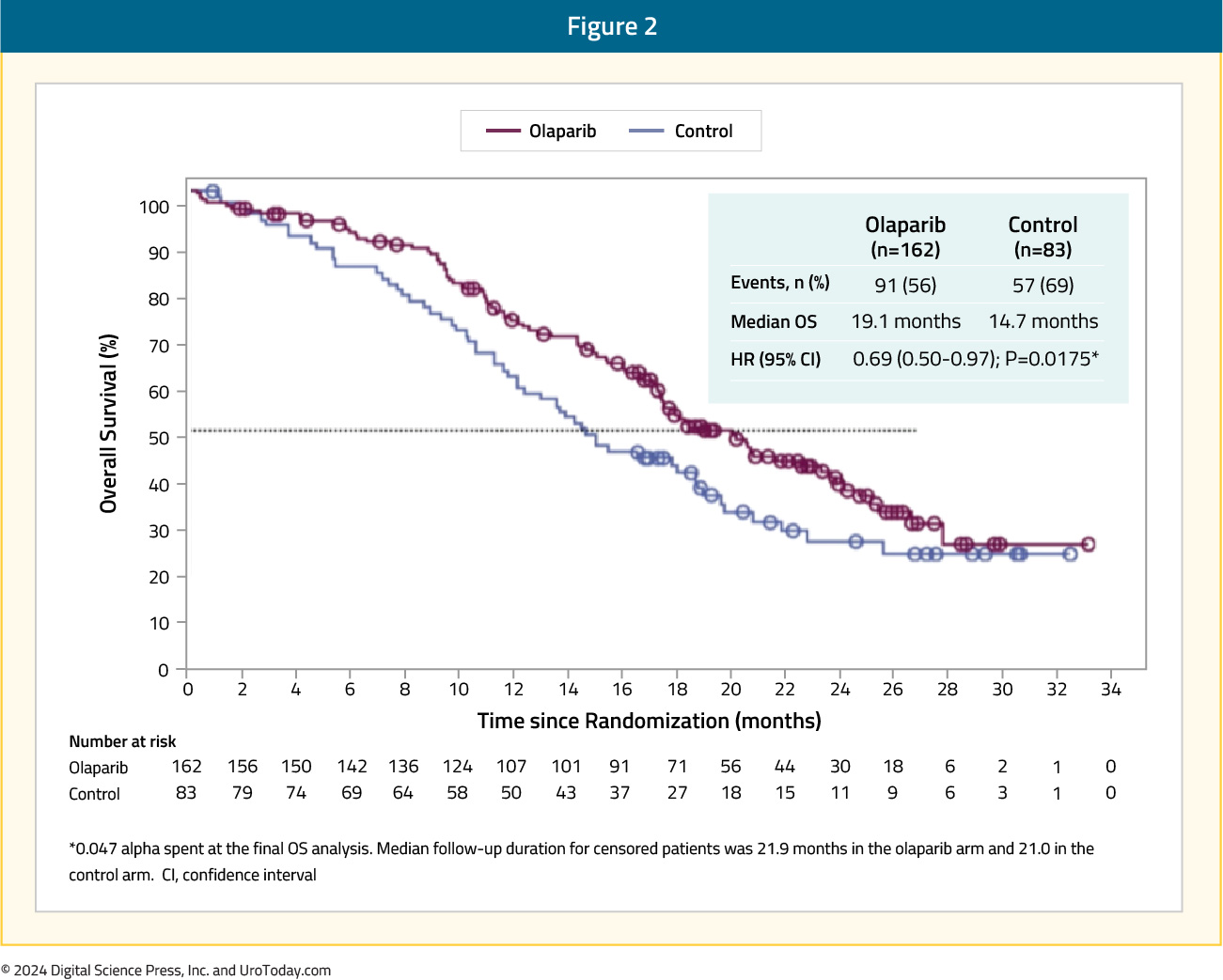
The data from PROfound formed the basis for the FDA-approval of olaparib 300 mg PO twice daily in men with HRR-mutated mCRPC after progression on enzalutamide or abiraterone.4
Rucaparib
The first PARP inhibitor to be approved by the FDA for the treatment of prostate cancer patients was rucaparib. On May 15, 2020, rucaparib was granted accelerated approval for patients with mCRPC and BRCA mutations (germline or somatic) who had progressed following treatment with androgen receptor-directed therapy and a taxane-based chemotherapy.3 This approval was based on the results of TRITON2, which was initially published in 202011 and most recently updated in 2023.12 TRITON2 is an international, open-label, phase II trial that evaluated the safety and efficacy of rucaparib 600 mg twice daily in mCRPC patients with DNA damage response (DDR) gene alterations who had progressed after 1–2 lines of an androgen receptor pathway inhibitor and one taxane-based chemotherapy. The efficacy cohort included 277 patients, of whom 172 (62.1%) had a deleterious germline or somatic BRCA alteration with 21.3%, 5.4%, 3.1%, 4%, and 4.7% having ATM, CDK12, CHEK2, PALB2, and other DDR gene mutations, respectively. A confirmed objective response was observed in 46% of BRCA patients with measurable disease (10% complete response). A superior response was observed among BRCA2 patients (48% versus 30% for BRCA1), which is potentially secondary to an increased frequency of biallelic mutations among BRCA2 patients and a greater coexistence of TP53 mutations among BRCA1-mutated men.13 The objective response was consistent irrespective of whether the BRCA mutation was somatic or germline and whether other DDR mutations were present or absent. All four patients with PALB2 mutations and measurable disease had an objective partial response, with none of the ATM-, CDK12-, CHEK2-mutated patients experiencing an objective response. A confirmed PSA50 response was observed in 53% and 55% of BRCA and PALB2-mutated patients, compared to 3.4–14% among patients with other DDR gene mutations. The median overall survival was 17.2 months for BRCA patients, compared to 11.1–14.6 months among ATM, CDK12, and CHEK2-mutated patients.
Following the promising results of TRITON2, the phase 3 TRITON3 trial was published in 2023. This was a randomized phase 3 trial of mCRPC patients with a BRCA1, BRCA2, or ATM alterations who experienced disease progression following treatment with a second-generation androgen receptor pathway inhibitor. Patients underwent 2:1 randomization to receive oral rucaparib (600 mg twice daily) or a physician’s choice control (docetaxel or a second-generation ARPI [abiraterone acetate or enzalutamide]). The primary outcome was the median PFS according to independent review. There were 405 patients randomized to receive rucaparib (n=270) or the control group (n=135). At 62 months follow-up, imaging-based PFS was significantly prolonged in the rucaparib group compared to the control group, both in the BRCA subgroup (11.2 and 6.4 months, respectively; HR: 0.50; 95% CI: 0.36 – 0.69) and in the intention-to-treat population (10.2 and 6.4 months, respectively; HR: 0.61; 95% CI: 0.47 – 0.80; p<0.001 for both comparisons). No significant PFS benefit was observed in the ATM subgroup.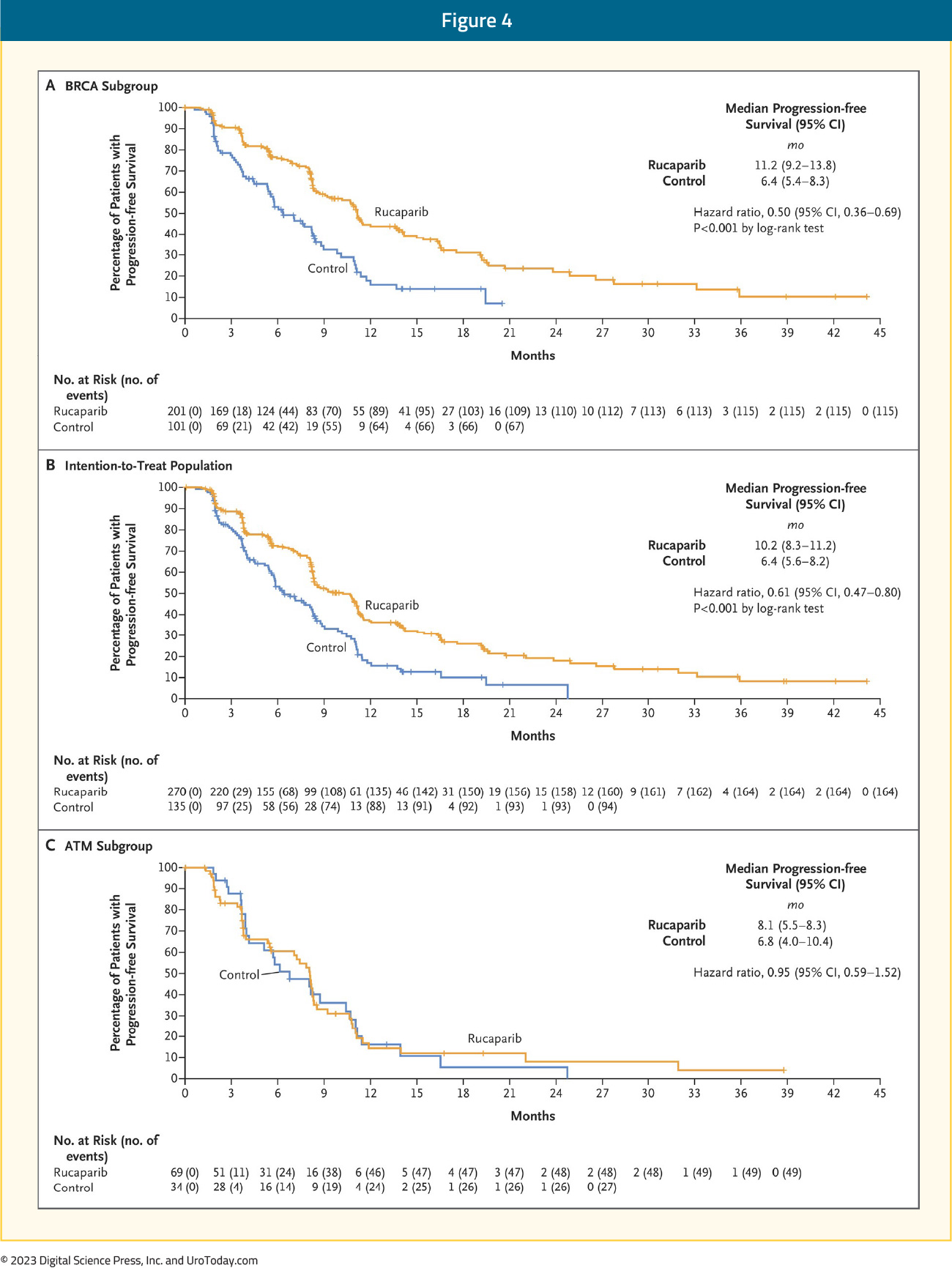
In the BRCA subgroup, the median OS was 24.4 versus 20.8 months in favor of rucaparib (HR: 0.81, 95% CI: 0.58 – 1.12, p=0.21).14
Talazoparib
TALAPRO-1 was an open-label, phase II trial that evaluated talazoparib 1 mg/day in patients with evidence of progressive mCRPC who had measurable soft-tissue disease and evidence of one of 11 DDR mutations who had progressed following taxane-based chemotherapy (48% both docetaxel and cabazitaxel) and abiraterone and/or enzalutamide (98% of population). The primary endpoint was confirmed ORR. There were 128 patients enrolled, of whom 127 received at least one dose of talazoparib (safety population) and 104 had measurable soft-tissue disease (antitumor activity population). After a median follow-up of 16.4 months, the ORR was 30% (95% CI: 21.2 – 39.6%).15
Niraparib
GALAHAD was a multicenter, open-label, single arm phase II trial of 289 mCRPC patients with DNA repair gene defects and disease progression following a prior next-generation androgen signaling inhibitor and a taxane, who received niraparib 300 mg orally once daily. The primary endpoint was ORR in patients with BRCA alterations and measurable disease. At a median follow-up of 10 months, the ORR in the measurable BRCA cohort was 34.2%. The median duration of objective response was 5.6 months. Conversely, the ORR in the measurable non-BRCA cohort was 10.6%. Median rPFS (8.1 versus 3.7 months) and OS (13.0 and 9.6 months) were both longer in the BRCA cohort, compared to the non-BRCA cohort.16
Management of Side Effects of PARP Inhibitors
The adverse event/safety profiles of all PARP inhibitors overlap considerably. The most common (any CTCAE grade) clinical side effects in phase III trials of rucaparib, olaparib and niraparib include:17
- Nausea: ~75%
- Fatigue: 60–70%
- Vomiting: ~35%
- Constipation: 20–40%
- Dysgeusia: 10–40%
- Anorexia: ~25%
- Abdominal pain: 25–30%
- Diarrhea: 20–30%
- Headache: 20–25%
- Cough: 10–15%
The most common (any CTCAE grade) lab abnormalities were:
- Anemia: 40–50%
- Thrombocytopenia: 15–60%
- Neutropenia: 20–30%
- Alanine aminotransferase (ALT) elevation: 5–36%
- Aspartate aminotransferase (AST) elevation: 2–28%
- Increased serum creatinine level: 10–15%
While nausea is the most common side effect of PARP inhibitor therapy, it tends to be mild in most cases. This side effect can be managed by taking the medication after a meal and an antiemetic (prochlorperazine or a 5-HT3 antagonist such as ondansetron) may be considered in patients who develop moderate or severe nausea and/or vomiting with PARP inhibitor therapy.
Close monitoring of patients following PARP inhibitor therapy initiation is required, particularly in the first three months, as hematologic adverse effects usually occur early, but not invariably, and regular blood counts should continue while patients are on treatment. Anemia is the most common hematologic toxicity observed with PARP inhibitors, with grade 3–4 anemia observed in 22% of patients on olaparib, 27% of patients on rucaparib, and 31% of patients on niraparib first-line maintenance therapy ovarian cancer trials.18-21 The management of such events may include dose reductions and/or interruptions, with transfusions reserved for symptomatic anemic events or if the hemoglobin level falls to <7 g/dL. Thrombocytopenia appears to be more common with niraparib at 61%, as opposed to olaparib (14%) or rucaparib (28%). The niraparib FDA label thus recommends obtaining weekly platelet levels during the first month of therapy.
Elevated serum creatinine level occurs within the first few weeks of therapy and is thought to be an on-target effect due to the inhibition of renal transporter proteins. Thus, serum creatinine-based estimation of renal function may be inaccurate in patients receiving PARP inhibitor therapy. Alternative methods of glomerular filtration rate (GFR) estimation such as radionuclide scan or serum-cystatin C must be used in cases where a more accurate GFR estimate is necessary. Elevation of AST and ALT also tends to typically occur within the first two cycles and can be transient. Treatment interruption may not be required for mild AST/ALT elevations, but serum bilirubin levels must be checked in all patients to evaluate for drug-induced liver injury.
Owing to their mechanism of action, there was a concern regarding treatment-emergent myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML) with PARP inhibitor therapies. However, it appears that the risk of MDS/AML is <1.5%. Of the 2,351 patients treated in olaparib monotherapy trials, only 28 (<1.5%) developed MDS/AML. Of these, 25/28 patients had a BRCA mutation, two patients had a wild-type germline BRCA, and one patient had unknown BRCA mutation status. The duration of olaparib varied from < 6 months to > 2 years and all had received previous chemotherapy with platinum and/or other DNA damaging agents, or radiotherapy.17 If pancytopenia occurs at any point during PARP inhibitor therapy, treatment must be interrupted as per guidelines for the drug, and appropriate evaluation for MDS and AML must be undertaken. Therapy must be discontinued permanently if a diagnosis of MDS or AML is confirmed.
Another important consideration is the potential for clinically-significant drug-drug interactions (DDI) with all PARP inhibitors. Rucaparib and olaparib are primarily metabolized by different members of the cytochrome P450 enzyme family, resulting in only a partial overlap in DDIs. Niraparib is metabolized in the liver by carboxylesterase-catalyzed amide hydrolysis with cytochrome P450 playing only a negligible role.22 Many commonly used drugs (such as phenytoin, carbamazepine, ketoconazole, ciprofloxacin, digoxin) have uni- or bi-directional interactions with PARP inhibitors. Thus, careful attention must be paid to minimize DDI by avoiding, discontinuing, adjusting the dose, or clinical/lab monitoring of these medications before and during PARP therapy. Involving a dedicated oncology pharmacist, where available, may be a valuable aid in this treatment setting.
Conclusions and Future Directions
PARP inhibitor monotherapy has demonstrated promising outcomes for the treatment of HRR-mutated mCRPC patients with evidence of disease progression following treatment with an androgen receptor pathway inhibitor and/or taxane-based chemotherapy. As a result, there has been an increased interest in ‘moving up’ these agents along the disease spectrum, as well as combining PARP inhibitors with other agents that may have a synergistic mechanism of action.
Published March 2024