Artificial intelligence continues to transform the field of medicine, including the management of prostate cancer. In this Center of Excellence article, we discuss the contemporary literature evaluating artificial intelligence for risk stratification after primary therapy, ADT treatment intensification, and evaluation of metastatic disease.
Artificial Intelligence for Prostate Cancer Risk Stratification After Primary Therapy
Arguably, the greatest efforts to date and the most impactful utilization of artificial intelligence has been in the space of prostate cancer risk stratification after primary therapy, both after biochemical recurrence following radical prostatectomy and radiation therapy.
Artificial Intelligence to Guide Treatment - Radical ProstatectomyAfter radical prostatectomy, one-third of patients will experience biochemical recurrence, which is associated with subsequent metastasis and cancer-specific mortality. Tan and colleagues1 have published results of their study using machine learning algorithms to predict biochemical recurrence after radical prostatectomy, comparing them with traditional regression models and nomograms. In this study, 18 clinicopathological parameters of 1,130 consecutive patients who underwent radical prostatectomy were recorded, yielding over 20,000 data points for analysis. The data set was split in a 70:30 ratio to training and validation sets, respectively, and was subsequently analyzed using three machine learning models: Naïve Bayes, random forest, and support vector machine. Over a median follow-up of 70.0 months, 176 (15.6%) men developed biochemical recurrence, at a median time of 16.0 months (IQR 11.0-26.0). The three machine learning models demonstrated good prediction of biochemical recurrence at 1, 3, and 5 years, with the area under curves of the Naïve Bayes model of 0.894, 0.876, and 0.894, respectively; of the random forest model of 0.846, 0.875, and 0.888, respectively; and of the support vector machine of 0.835, 0.850, and 0.855, respectively. All models demonstrated robust accuracy (>0.82), good calibration with minimal overfitting, longitudinal consistency across the three time points, and inter-model validity. The machine learning models were also comparable to traditional regression analyses (which had an area under the curve of 0.797, 0.848, and 0.862 at 1, 3, and 5 years, respectively) and outperformed the three nomograms: Kattan (area under the curve: 0.815, 0.798, and 0.799), JHH (area under the curve: 0.820, 0.757, and 0.750) and CAPSURE nomograms (area under the curve: 0.706, 0.720, and 0.749) (p < 0.001). Based on this early work assessing biochemical recurrence after radical prostatectomy, machine learning algorithms may facilitate tailored care by identifying high-risk patients who will benefit from multimodal therapy. Further, it may allow identification of patients at particularly low risk of recurrence who may benefit both psychologically from knowing this and from a reduced intensity surveillance schedule.
Artificial Intelligence to Guide Treatment - RadiotherapyOver the last several years, our radiation oncology colleagues have performed beautiful work across several studies evaluating the utility of artificial intelligence in risk stratification among men undergoing primary radiotherapy. Machine learning holds great promise for impacting healthcare delivery, however most methods are tested in 'simulated' environments that cannot recapitulate factors influencing real-world clinical practice. As such, McIntosh et al.2 from the University of Toronto prospectively developed and evaluated a random forest algorithm for therapeutic curative-intent radiation therapy treatment planning for prostate cancer in a blinded, head-to-head study with full integration into the clinical workflow:

Machine learning- and human-generated radiation therapy treatment plans were directly compared in a retrospective simulation with retesting (n = 50) and a prospective clinical deployment (n = 50) phase. The machine learning model training pipeline consisted of four phases: (i) feature extraction, (ii) atlas regression forest training, (iii) accuracy estimation, and (iv) atlas selection learning:

Throughout the study phases, treating physicians assessed machine learning- and human-generated radiation therapy treatment plans in a blinded manner, with the selected radiation therapy plan in the prospective phase delivered for patient treatment. Overall, 89% of machine learning-generated radiation therapy plans were considered clinically acceptable and 72% were selected over human-generated radiation therapy plans in head-to-head comparisons. Furthermore, radiation therapy planning using machine learning reduced the median time required for the entire radiation therapy planning process by 60.1% (from 118 hours to 47 hours).
Decades ago, the RTOG group set up a biobank that acted as a repository of clinical, pathologic, and imaging data from numerous trials, including RTOG 9202, 9413, 9910, 0126, and 9408. Using clinical data from over 5,000 patients with over 16,000 H&E pathologic specimens available, multimodal artificial intelligence has been used to develop a prognostic risk score that can predict the risk of various oncologic outcomes, including 5- and 10-year biochemical failure, distant metastasis, prostate cancer-specific and overall mortalities. As follows are several of the studies that have been published from this collaborative endeavor.
Previously presented at the 2022 GU ASCO annual meeting and subsequently published in NPJ Digital Medicine,3 Dr. Osama Mohamad’s group led an initiative to develop accurate and scalable tools to support therapy personalization with prognostic biomarkers. In this key study, they were able to personalize prostate cancer therapy by predicting long-term, clinically relevant outcomes using a multimodal deep learning architecture, training models using clinical data and digital histopathology from prostate biopsies. Models were trained and validated using the aforementioned five phase III randomized RTOG trials, of which histopathological data was available for 5,654 of 7,764 randomized patients (71%) with a median follow-up of 11.4 years. The multimodal architecture is composed of two parts: a tower stack to parse a variable number of digital histopathology slides and another tower stack to merge the resultant features and predict binary outcomes:

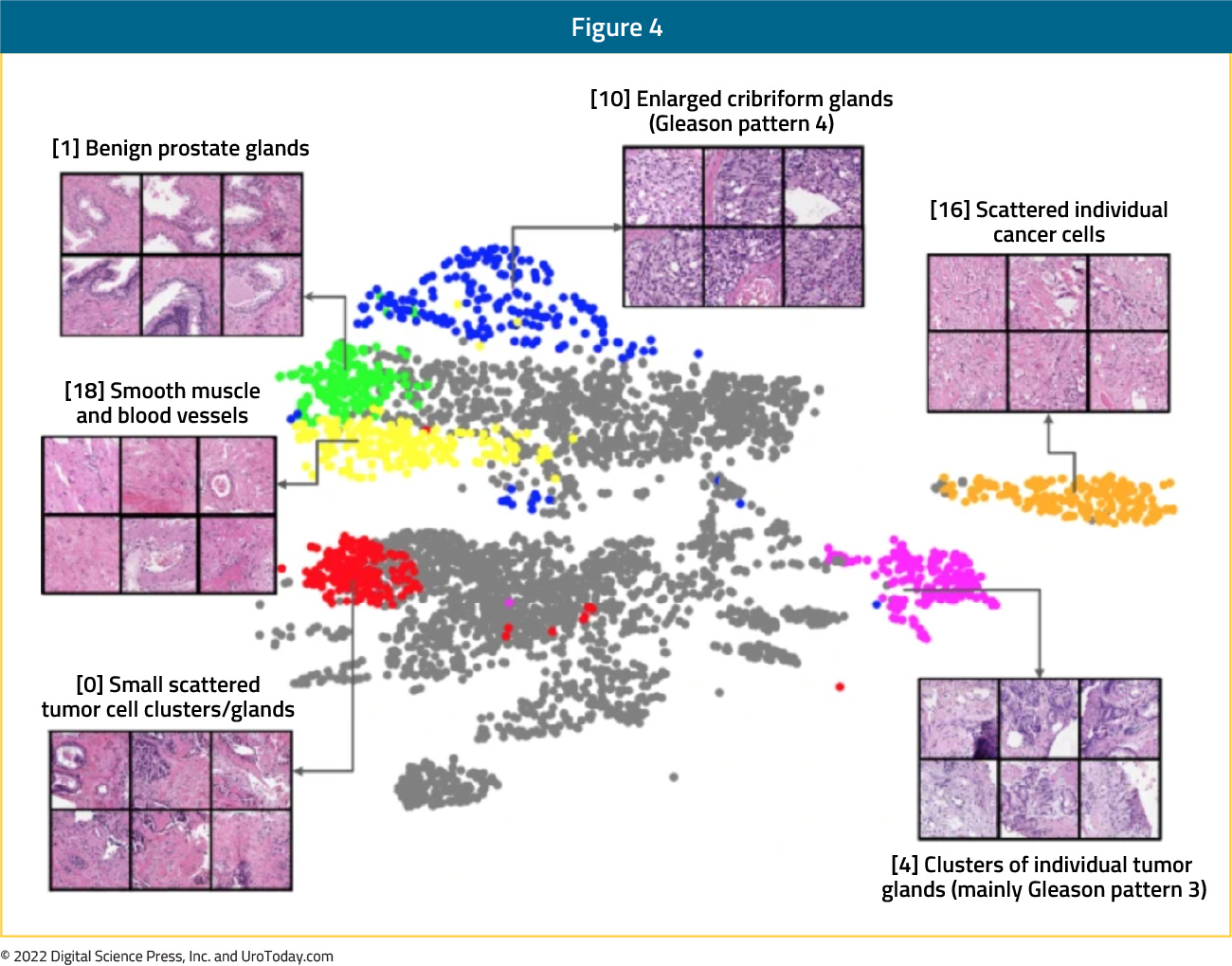
The self-supervised model in the multimodal model was trained to identify whether or not augmented versions of small patches of tissue came from the same original patch, without ever seeing clinical labels. After training, each image patch in the dataset was fed through this model to extract a 128-dimensional feature vector, and the UMAP algorithm was used to cluster and visualize the resultant vectors. Subsequently, a pathologist then asked to interpret the 20 image patches closest to each of the 25 cluster centroids (6 representative patches shown):
Compared to the most common risk-stratification tool-risk groups developed by the NCCN, these models had superior discriminatory performance across all endpoints, ranging from 9.2% to 14.6% relative improvement in a held-out validation set. This artificial intelligence-based tool (called ArteraAI) improved prognostication over standard tools and allows oncologists to computationally predict the likeliest outcomes of specific patients to determine optimal treatment:

At ASTRO 2022, Dr. Jonathan Tward presented work demonstrating that a multi-modal artificial intelligence model could stratify patients into risk groups that more precisely and accurately reflect their prognosis compared to D’Amico/NCC risk groups. In this analysis of 5,569 patients in the five RTOG phase 3 trials with a median follow-up of 11.4 years, patients were stratified into deciles (N=557/decile) based on their multi-modal artificial intelligence prognostic scores. The risk of metastasis by decile was determined using competing risk regression models, and deciles were grouped into 3 cohorts based on risk of metastasis by 10 years:
- Multi-modal artificial intelligence low: <10%
- Multi-modal artificial intelligence medium: 10-25%
- Multi-modal artificial intelligence high: >25%
The multi-modal artificial intelligence decile scores demonstrated that the lowest six deciles were associated with a low risk of distant metastasis (<10%), the next three were associated with a medium risk (10-25%), whereas the highest decile group was the only one associated with a high risk of >25%:

Furthermore, among the 3,342 patients in the multi-modal artificial intelligence low group, 76% of patients were intermediate risk, with only 16% of patients in this group falling into the NCCN low risk category. In the multi-modal artificial intelligence medium group of 1,671 patients, 67.7% were NCCN high-risk:

However, it appears that the risk of metastasis in the multi-modal artificial intelligence and NCCN low groups are similar, given that the 10-year risk of distant metastasis in the NCCN and multi-modal artificial intelligence low risk groups is 3% in both groups. The corresponding rates in the medium risk groups was 12% in the multi-modal artificial intelligence medium and 6% in the NCCN intermediate. Notably, within the multi-modal artificial intelligence high group, the risk of 10-year metastasis in radiation-treated patients is 60% in NCCN intermediate risk (n=15) and 36% in NCCN high/very high risk (n = 540). This is likely due to differences in the number of patients in each of these subgroups, as well as the fact that 96% of patients in the NCCN high/very high group received concurrent ADT:

Notably, multi-modal artificial intelligence identified 6-fold more patients than NCCN with the lowest risk of metastasis:

Artificial Intelligence for ADT Treatment Intensification
At the 2022 GU ASCO annual meeting, Dr. Daniel Spratt discussed an artificial intelligence-derived digital pathology-based biomarker to predict the benefit of ADT in localized prostate cancer with validation in NRG/RTOG 9408 trial. Of note, the current standard of care for men with intermediate- and high-risk localized prostate cancer treated with radiotherapy is the addition of ADT. However, this will prove to be overtreatment for many men who will not realize any benefit but will experience toxicity. Thus far, we are unable to reliably identify those men who do and do not benefit from this treatment intensification.
Prognostic biomarkers estimate the absolute risk of recurrence and can assist with personalizing treatment through avoiding futile treatment intensification. However, more usefully, predictive biomarkers identify the relative impact of a given therapy and personalize treatment decisions irrespective of prognosis. Presently, there are no validated predictive biomarkers to guide ADT use or duration in such men. However, there is a wealth of unused biological information unrecognized in prostate cancer histopathology. Use of artificial intelligence may identify features that are unidentifiable or uninterpretable to even expert human pathologists, enabling the creation and validation of the first predictive biomarker to guide ADT use in localized prostate cancer patients.
In the work discussed by Dr. Spratt at GU-ASCO 2022, pre-treatment biopsy slides were digitized from the aforementioned five phase III NRG Oncology randomized trials of men receiving radiotherapy with or without ADT. The training set used to develop the artificial intelligence-derived predictive biomarker included NRG/RTOG 9202, 9413, 9910, and 0126, and was trained to predict distant metastasis. A multimodal deep learning architecture was developed to learn from both clinicopathologic and digital imaging histopathology data and identify differential outcomes by treatment type. After the model was locked, an independent biostatistician performed validation on NRG/RTOG 9408, a phase III randomized trial of radiotherapy +/- 4 months of ADT:

The distant metastasis rates were calculated using cumulative incidence functions in biomarker positive and negative groups, and the biomarker-treatment interaction was assessed using Fine-Gray regression wherein death without distant metastasis was treated as a competing event.
Clinical and histopathological data were available for 5,654 of 7,957 eligible patients (71.1%) across the five clinical trials. The training cohort included 3,935 patients and had a median follow-up of 13.6 years (IQR 10.2, 17.7). After the artificial intelligence-derived predictive ADT classifier was trained, it was validated in NRG/RTOG 9408 (n = 1719, median follow-up 17.6 years, IQR 15.0, 19.7). Importantly, the multimodal artificial intelligence predictive model was primarily driven by digital histopathology:

In the NRG/RTOG 9408 validation cohort that had digital histopathology data, ADT use significantly improved distant metastasis (HR 0.62, 95% CI 0.44, 0.87), consistent with the published trial results. The biomarker-treatment interaction was significant (p = 0.0021). Notably, in patients with artificial intelligence-biomarker positive disease (n = 673, 39%), there was a significant benefit to the addition of ADT to radiotherapy (HR 0.33, 95% CI 0.19, 0.57). Conversely, in the biomarker negative subgroup (n = 1046, 61%), the addition of ADT did not improve outcomes over radiotherapy alone (HR 1.00, 95% CI 0.64, 1.57). The 15-year distant metastasis rate difference between radiotherapy versus radiotherapy + ADT in the biomarker negative group was 0.4% compared to 9.8% in the biomarker positive group. Additionally, there was a consistent differential benefit seen by the biomarker score across all endpoints:

This study represented the first predictive biomarker of ADT benefit with radiotherapy in localized intermediate risk prostate cancer using a novel artificial intelligence-derived digital pathology-based platform. Importantly, a majority of patients treated with radiotherapy in the NRG/RTOG 9408 trial did not require concurrent ADT and could have avoided both the cost and the side effects of such treatment intensification. Moving forward, perhaps this technology will enable personalization of care among localized prostate cancer patients undergoing local radiotherapy.
Artificial Intelligence and the Evaluation of Metastatic Disease
Understanding treatment patterns and effectiveness for patients with metastatic prostate cancer is dependent on accurate assessment of metastatic status. At the population level, methods to identify patients diagnosed with metastatic prostate cancer is difficult given that cancer registries provide detailed data at diagnosis but are not updated throughout the natural history and progression of the disease. In a recently published study, Yang et al.4 developed a natural language processing model with machine learning for identifying patients with metastatic prostate cancer, evaluating the model’s performance against chart-reviewed data and an ICD 9/10 code-based method. For this study, 139,057 radiology reports on 6,211 unique patients from the Department of Veterans Affairs were used. When compared with chart review, the natural language processing model had high sensitivity (85%) and specificity (96%). Additionally, the natural language processing model was able to predict patient-level metastasis status with a sensitivity of 91% and specificity of 81%, whereas sensitivity and specificity using ICD9/10 billing codes were 73% and 86%, respectively. The area under the curve for the natural language processing model was 0.911.
The Bone Metastases Ensemble Trees for Survival (BMETS) model is a model that uses a machine learning algorithm to estimate survival time following consultation for palliative radiation therapy for symptomatic bone metastases. To validate this model, Elledge and colleagues5 assessed 216 sites of symptomatic bone metastases in 182 patients (of whom 23% were prostate cancer patients) in a tertiary-care, academic medical center. When the BMETS model was applied to the external data set, time-dependent area under the curve values at 3, 6, and 12 months were 0.82, 0.77, and 0.77, respectively. Additionally, when refit with data from the combined training and external validation sets, the time-dependent area under the curve values remained > 0.79.
Conclusions
The utilization of artificial intelligence and machine learning has demonstrated considerable promise in guiding treatment decisions for patients with prostate cancer, in particular, for risk stratification after primary therapy, in assessing the need for treatment intensification with concurrent ADT in patients receiving radiotherapy for localized prostate cancer, and for evaluation of metastasis among patients with advanced prostate cancer. The future of artificial intelligence has the potential to leverage and integrate the increasingly complex data collected during the prostate cancer journey in order to improve prognostication and treatment selection. Data from initial risk stratification based on modern prediction models can be integrated within artificial intelligence systems. In addition, tumor profiling using sequencing of tissue or circulating tumor DNA may be integrated to predict prognosis and optimize treatment:6
- Zachary Klaassen, MD MSc, Medical College of Georgia, Augusta, Georgia, USA
- Rashid K. Sayyid, MD MSc, University of Toronto, Toronto, ON
Published: April 2023