Bladder cancer remains the sixth most commonly diagnosed cancer in the United States, with an estimated 82,290 incident cases in 2023.1 Because of the persistent recurrence risk of NMIBC in a highly comorbid population, there has been an FDA-led drive towards developing novel treatment options for these patients. The following article will highlight recent advances in this disease space with a specific focus on the oncolytic adenovirus agent cretostimogene grenadenorepvec, and the registration trial in intermediate risk non-muscle invasive bladder cancer (NMIBC), PIVOT-006.
Cretostimogene Grenadenorepvec
Cretostimogene grenadenorepvec is a highly immunogenic expressing oncolytic adenovirus, and its oncolytic immunotherapy mechanism is that it encodes GM-CSF with insertion of the human EF2-1 promoter:
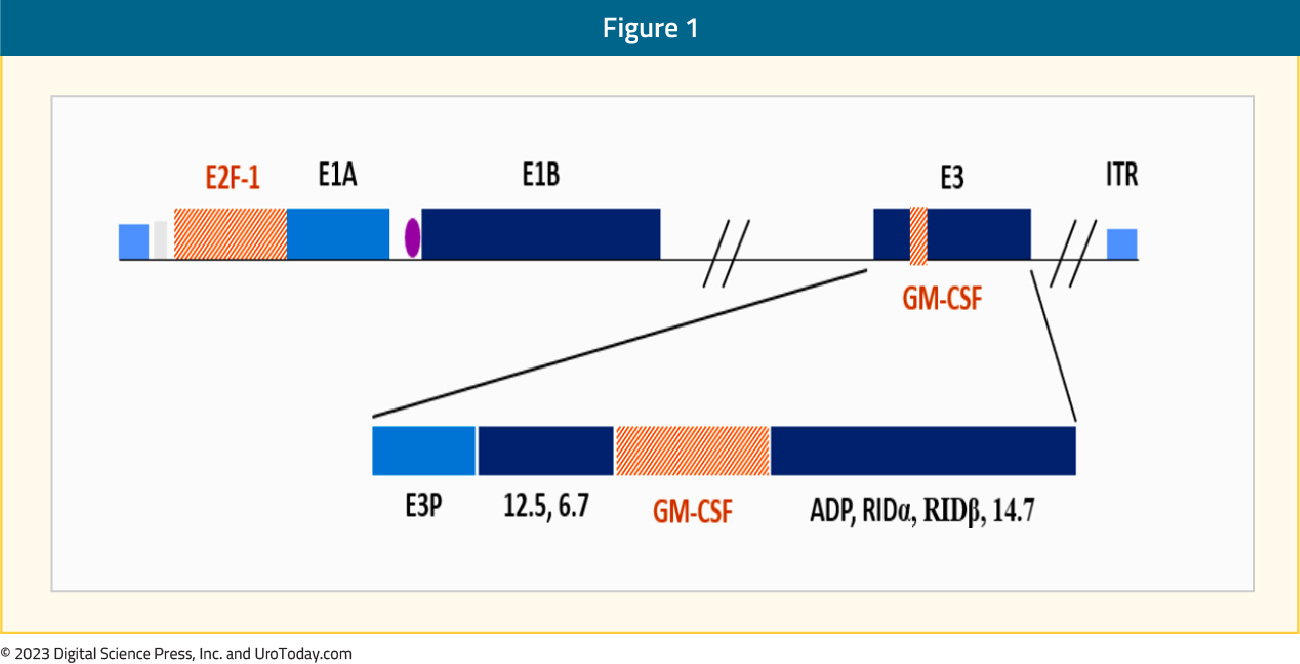
Cretostimogene binds to the Coxsackie Adenovirus Receptor leading to robust expression in all stages of bladder cancer, with subsequent viral replication leading to tumor lysis.
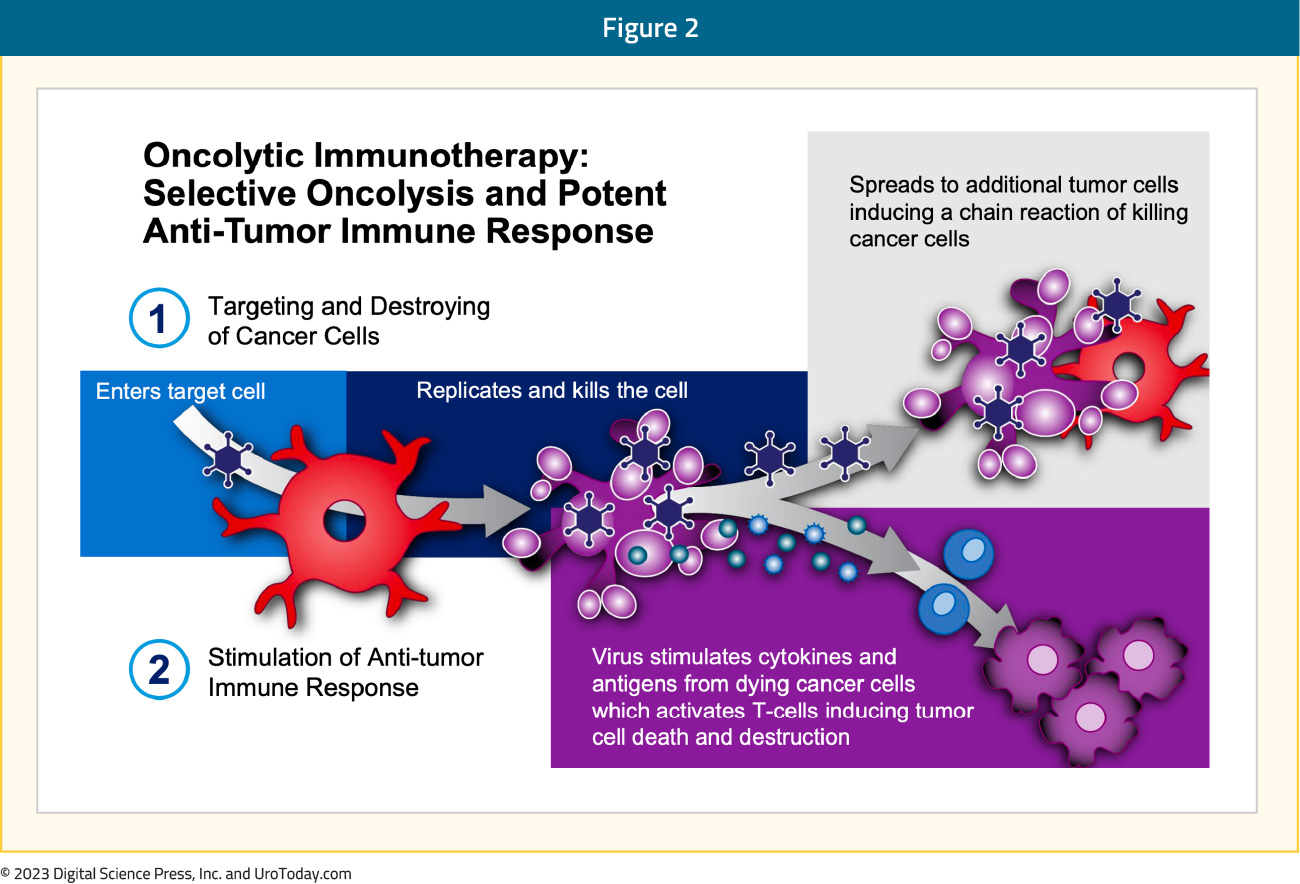
Oncolytic immunotherapy encompasses selective oncolysis and a potent antitumor response, with the following steps:
- Targeting and destroying cancer cells
- Stimulation of an anti-tumor response
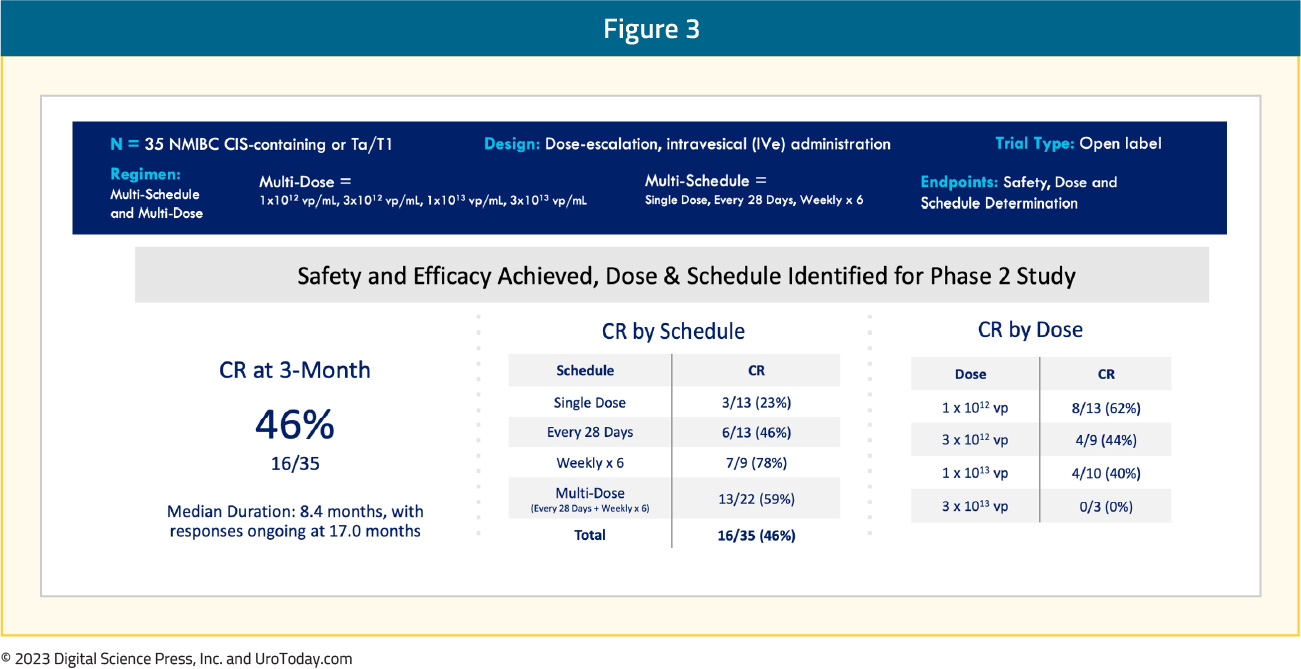
Cretostimogene grenadenorepvec monotherapy has previously been evaluated in a phase 1 trial (V0046) of 35 patients with high-risk, BCG-failure NMIBC (CIS-containing or papillary). Cretostimogene demonstrated a complete response rate of 46% at 3 months and met the safety/efficacy outcomes, with the target dose and schedule identified for a subsequent phase 2 study:2
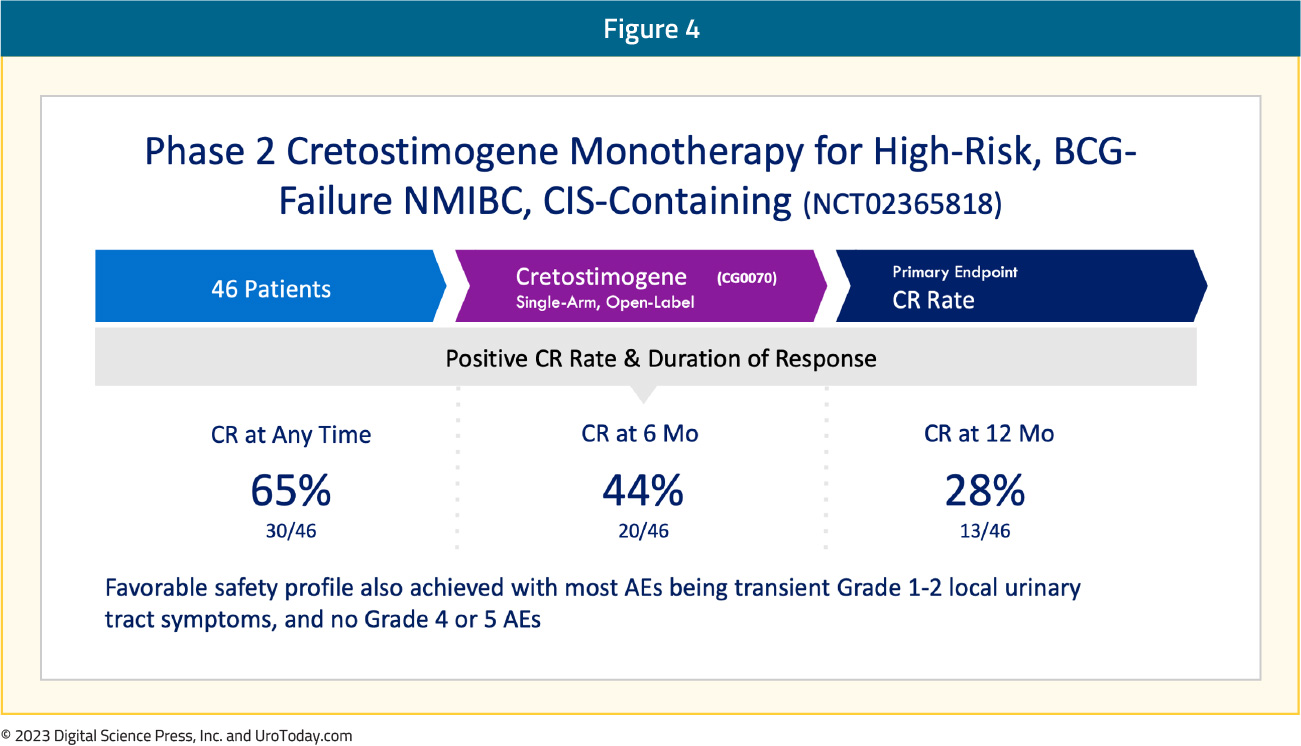
Next, cretostimogene grenadenorepvec monotherapy was evaluated in an open label, phase 2 trial (BOND-002) of 46 patients with BCG-failure NMIBC (containing CIS). A complete response at any time was achieved in 30/46 patients (65%), with durable complete responses of 44% and 28% at 6 and 12 months, respectively:3
Key Trials Featuring Cretostimogene Grenadenorepvec: CORE-001
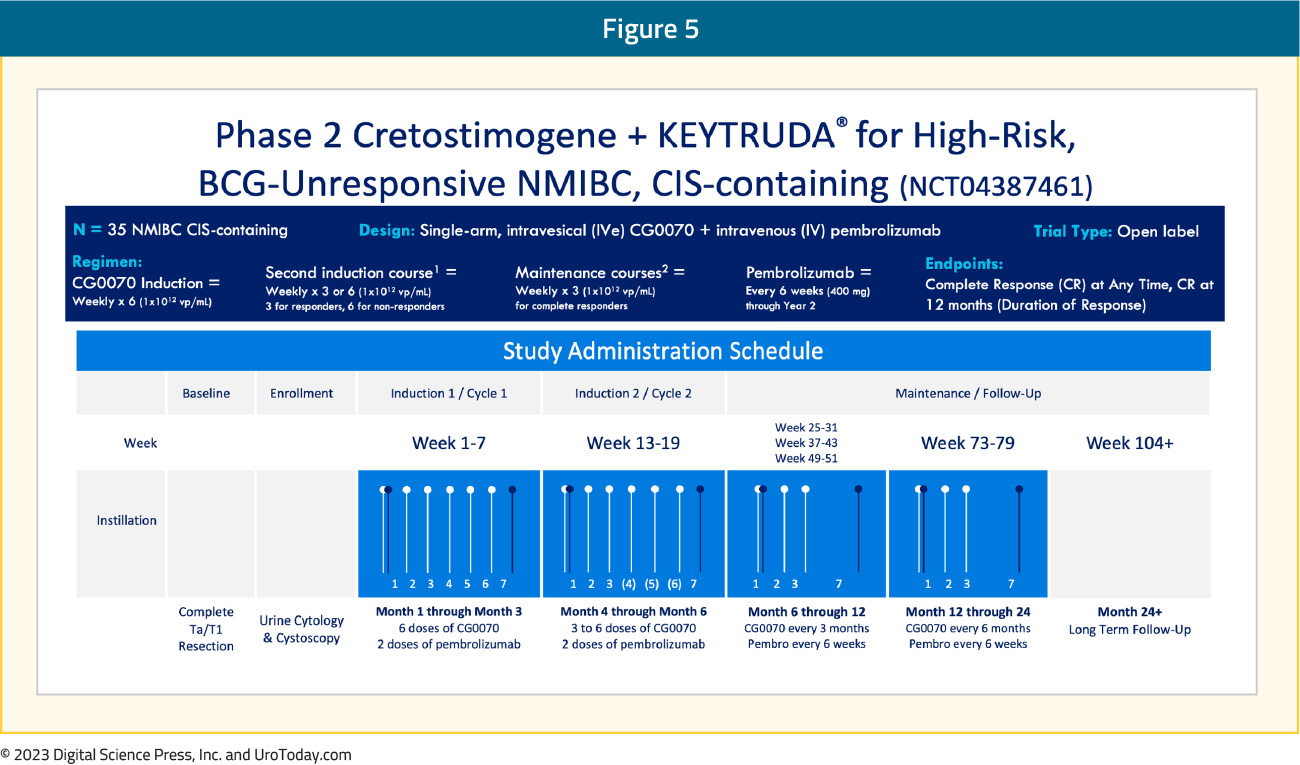
CORE-001 is a phase 2, single arm study of cretostimogene grenadenorepvec combined with pembrolizumab in patients with NMIBC unresponsive to intravesical BCG. CORE-001 evaluated 35 patients receiving cretostimogene induction weekly (1x1012 vp/mL) for 6 weeks, followed by a second induction course weekly for 3 weeks in responders and 6 weeks in non-responders. All responders subsequently received a maintenance course weekly for 3 weeks. Patients concurrently received pembrolizumab every 6 weeks (as opposed to the usual 3 weeks) at a dose of 400 mg through year 2. The study endpoints were complete response at any time and 12 months (duration of response):
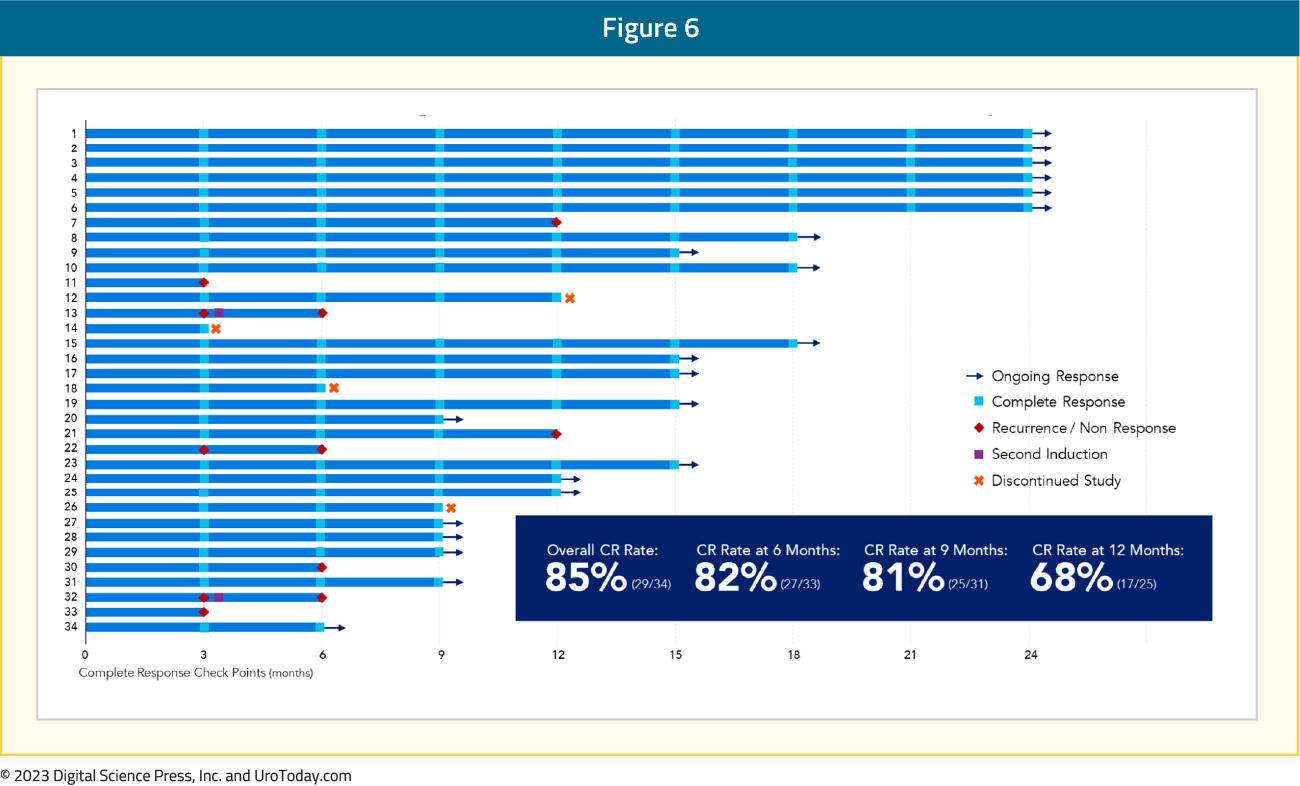
The median number of prior BCG instillations was 12 (range: 9 – 30), and 60% had persistent high-risk NMIBC, with the remaining 40% having recurrent high-risk NMIBC. Of note, 80% of patients had pure CIS. The swimmer’s plot for the study subjects shows an overall complete response rate of 85%, which was longitudinally maintained with 6-, 9-, and 12-month complete response rates of 82%, 81%, and 68%, respectively.
With regards to adverse events:
- Predominantly transient, grade 1-2 local GU AEs
- Grade 3 adverse events were observed in 4 patients (11%)
- No grade 4-5 adverse events were observed
- The adverse event profile was generally consistent with prior studies of each agent alone
- No clear evidence of additive/synergistic toxicity
Thus, this trial showed us that monotherapy activity of cretostimogene in NMIBC after BCG failure is achievable, and that the combination of cretostimogene and pembrolizumab appears to be highly active in BCG-unresponsive NMIBC based on these preliminary results.
Key Trials Featuring Cretostimogene Grenadenorepvec: BOND-003
BOND-003 is a phase 3 trial of intravesical Cretostimogene grenadenorepvec monotherapy for patients with high-risk BCG- unresponsive NMIBC with CIS. The trial is single-arm, open-label, with the intravesical administration of cretostimogene monotherapy for patients with pathologically confirmed BCG-unresponsive high-risk NMIBC with CIS +/- Ta/T1. Patients had all Ta/T1 disease resected prior to treatment, with mandatory biopsies at the 12-month assessment. The dosing regimen is an induction course of six weekly treatments, with the option for a second induction of six weekly treatments for non-responders. The maintenance course is weekly x 3 every 3 months for year 1 and then weekly x 3 every 6 months for year 2. The endpoints for the trial are complete response at any time, complete response at 12 months, duration of response, progression free survival, and recurrence free survival.
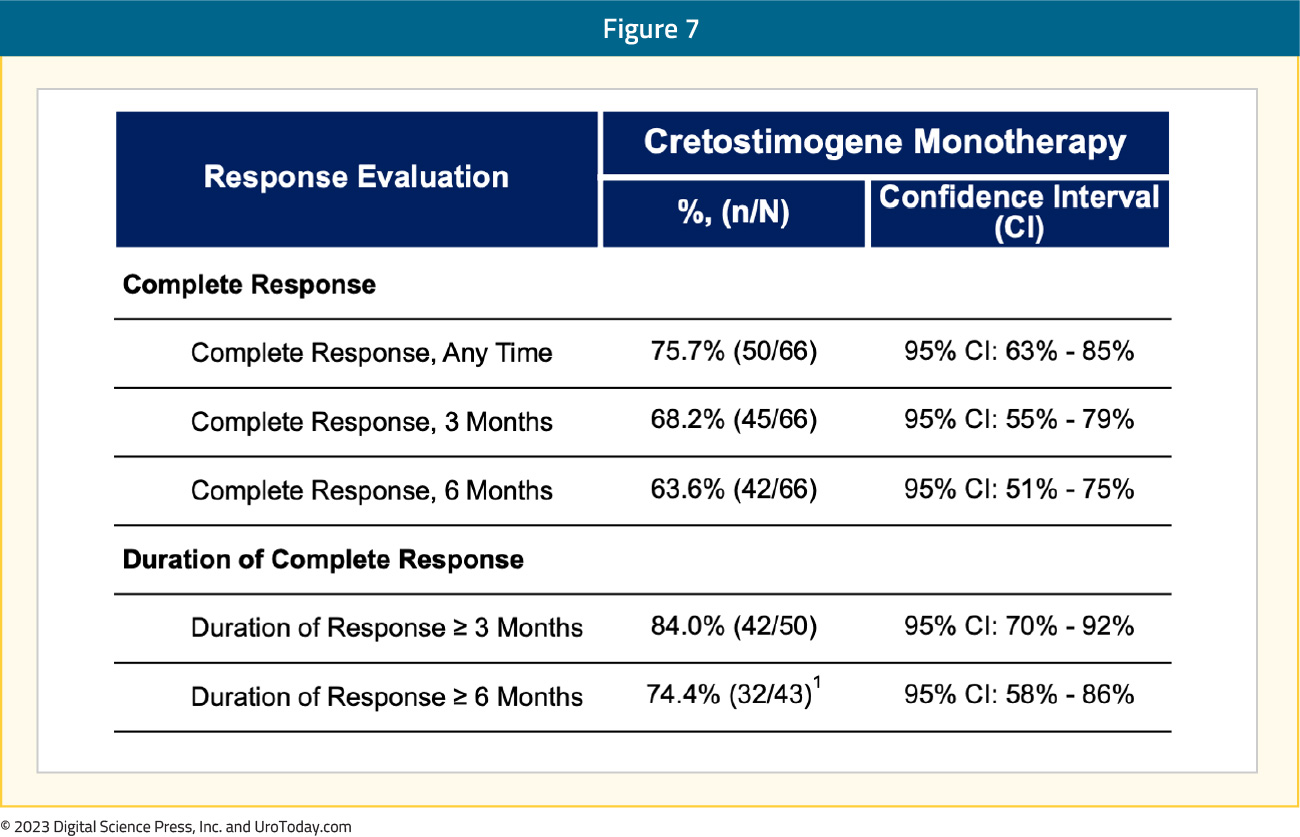
Among 66 patients evaluable (October 5, 2023), the majority of patients are male (76%), white (56%), and older than 65 years of age (80%). ECOG status was primarily 0 (80%), with the majority having previously received TICE BCG (83%). Of note, this was a very heavily pretreated cohort with 14 median number of BCG instillations (range: 7-47). The first results from BOND-003 included a 75.7% (95% CI 63% - 85%) complete response rate at any time based on central review. This in the context of all patients having active disease at baseline prior to enrollment and having received adequate BCG therapy as per FDA 2018 Guidance on BCG-unresponsive NMIBC. Additionally, 74.4% (95% CI 58% - 86%) (32/43) of responders maintained a response for >= 6 months. Full complete response and duration of complete response data are as follows:
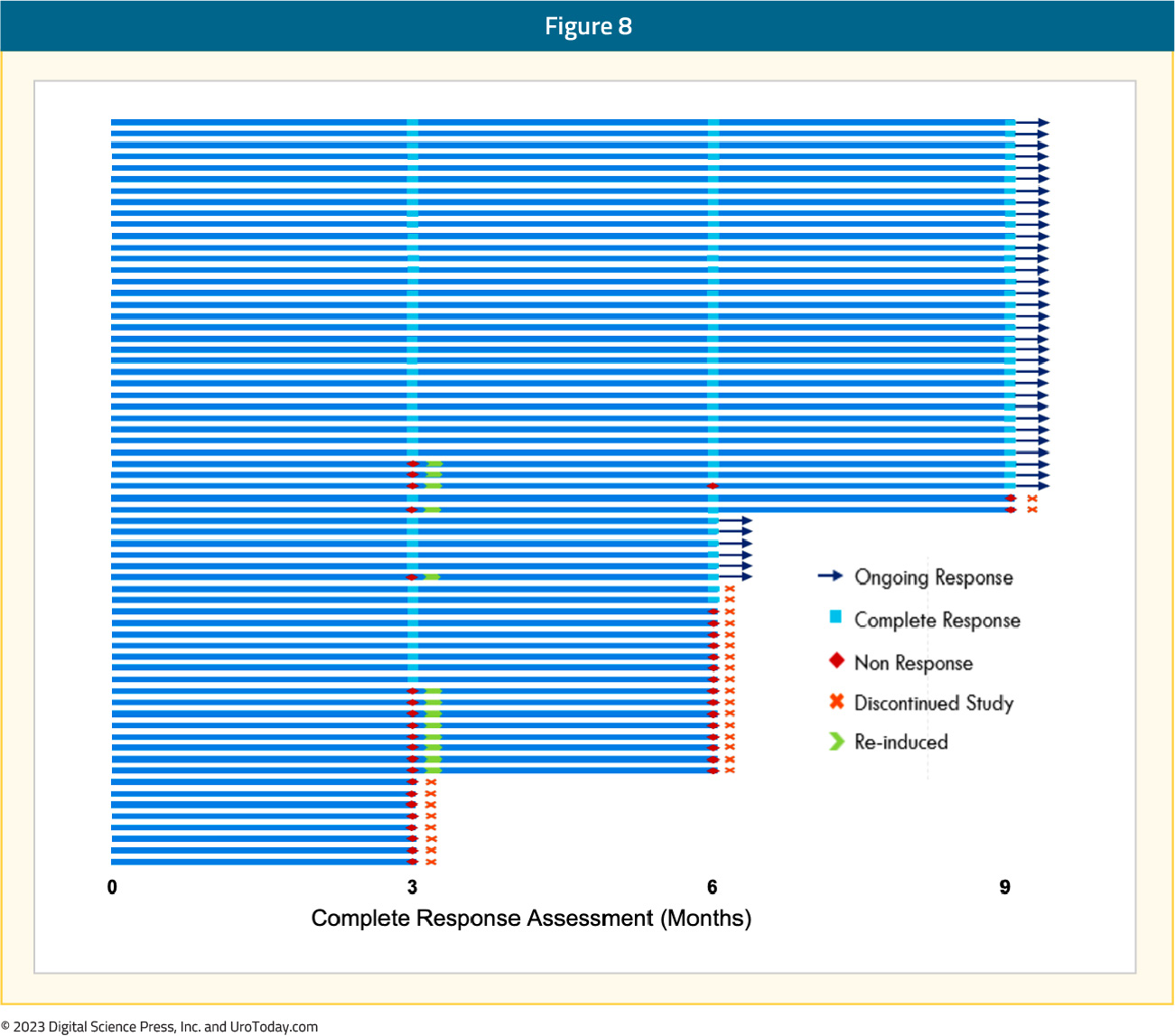
Cretostimogene also showed durable response over time with 31% of patients that were not initial responders being salvaged with re-induction. The Swimmer’s plot for this trial is as follows:
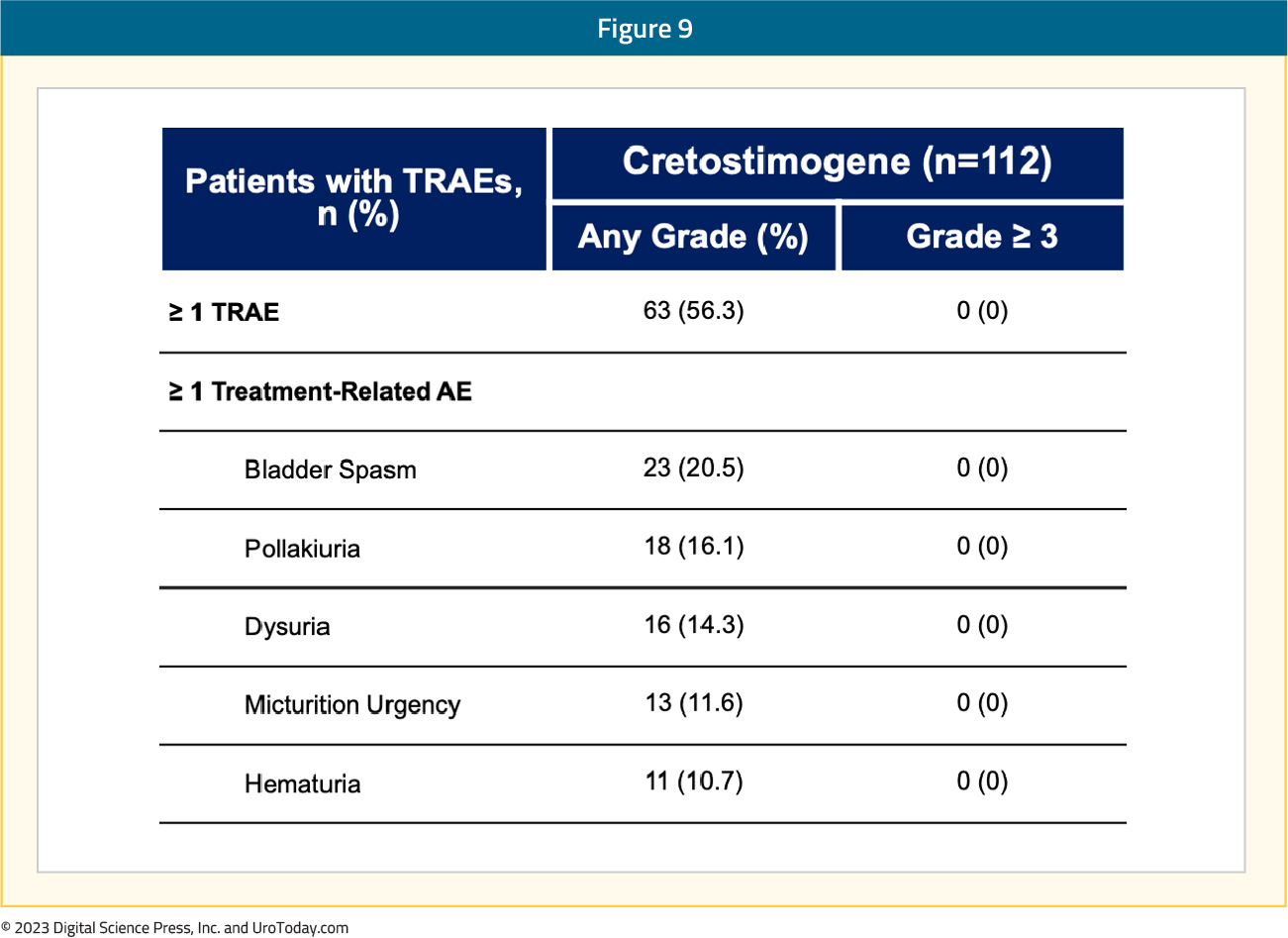
Cretostimogene has been generally well tolerated, with most adverse events being grade 1-2, with 2 patients (1.8%) having serious treatment-related adverse events (grade 2). There were no grade >= 3 treatment-related adverse events reported, no treatment discontinuations due to adverse events, and no deaths were reported:
BOND-003 has been granted FDA fast track designation for cretostimogene monotherapy in BCG-unresponsive CIS with or without Ta/T1 papillary disease.
Expansion of Cretostimogene Grenadenorepvec: Intermediate Risk
There is a significant unmet need with a high prevalence of intermediate-risk non-muscle invasive bladder cancer in the United States. At disease presentation, 75% have non-muscle invasive bladder cancer, of which there is the following breakdown:
- Low risk: ~30%
- Intermediate risk: ~30%
- High risk: ~40%
Intermediate risk non-muscle invasive bladder cancer has a high risk of recurrence (50%-70%), low risk of progression (<5%), is costly, common, chronic, and is associated with risks of anesthesia and surgery from multiple TURBTs.
The AUA risk stratification for intermediate risk disease is as follows:
- Low grade urothelial carcinoma:
- T1, or
- >3 cm, or
- Multifocal, or
- Recurrence with 1 year
- High grade urothelial carcinoma:
- Ta, and
- <=3 cm, and
- Solitary
According to the NCCN guidelines, the preferred treatment for intermediate risk NMIBC is intravesical therapy or surveillance. Additionally, the AUA has several treatment recommendations:
- In an intermediate-risk patient, a clinician should consider administration of a six-week course of induction intravesical chemotherapy or immunotherapy (Moderate Recommendation; Evidence Strength: Grade B)
- In an intermediate-risk patient who completely responds to an induction course of intravesical chemotherapy, a clinician may utilize maintenance therapy (Conditional Recommendation; Evidence Strength: Grade C)
- In an intermediate-risk patient who completely responds to induction BCG, a clinician should consider maintenance BCG for one year, as tolerated (Moderate Recommendation; Evidence Strength: Grade C)
PIVOT-006
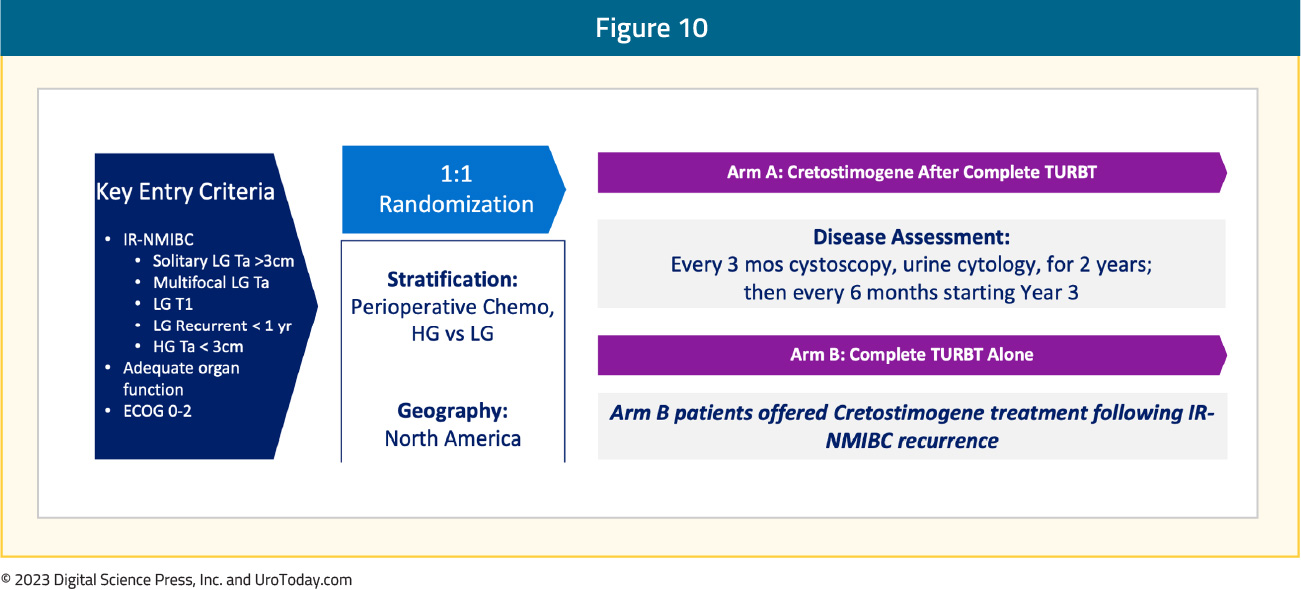
PIVOT-006 is a phase 3 open label, North American trial of adjuvant cretostimogene versus TURBT alone in intermediate risk NMIBC. The expected recruitment for this trial is up to 426 participants who will be randomized to either intravesical cretostimogene after TURBT versus TURBT alone. The key inclusion criteria are:
- Intermediate risk NMIBC per the AUA/SUO 2020 definition which is pathologically confirmed within 12 weeks of the study start
- All visible disease removed by TURBT within 12 weeks of randomization
- 18 years of age or older
- ECOG performance status 0-2
- Willing to use barrier contraception 14 days prior to and 6 weeks post cretostimogene doses
- Willing to comply with study mandated procedures
- Prior high grade NMIBC is permitted, if intermediate NMIBC is present at study entry
- Prior BCG and intravesical chemotherapy is permitted, after a washout period
The key exclusion criteria are:
- Current or prior evidence of high risk NMIBC (high grade T1, high grade Ta >3 cm that is recurrent or multifocal, any CIS, any variant histology, any high grade prostatic urethra involvement, any LVI, any BCG treatment failure in high grade patients)
- Has intermediate risk NMIBC that cannot be completely resected
- Low risk NMIBC (low grade solitary Ta <= 3 cm that has recurred more than 12 months after a previous high grade or low grade tumor). No low grade, low risk disease
- Has a history of current muscle invasive bladder cancer (T2 or higher stage), locally advanced (T3/T4, any N) or metastatic disease
Stratification factors will be receipt of perioperative chemotherapy and high versus low grade intermediate risk disease. Disease assessment will be an every 3 month cystoscopy and urine cytology for 2 years and then every 6 months starting in year 3. Imaging will be every 12 months and pathology will be centrally reviewed. Importantly, control arm patients will be offered cretostimogene treatment following intermediate risk NMIBC recurrence. The trial schema for PIVOT-006 is as follows:
The key endpoints for the trial are:
- Recurrence free survival (without recurrence or progression in the bladder, upper tract, or prostatic urethra)
- Recurrence free survival at 12 months and 24 months
- Progression free survival
- Safety
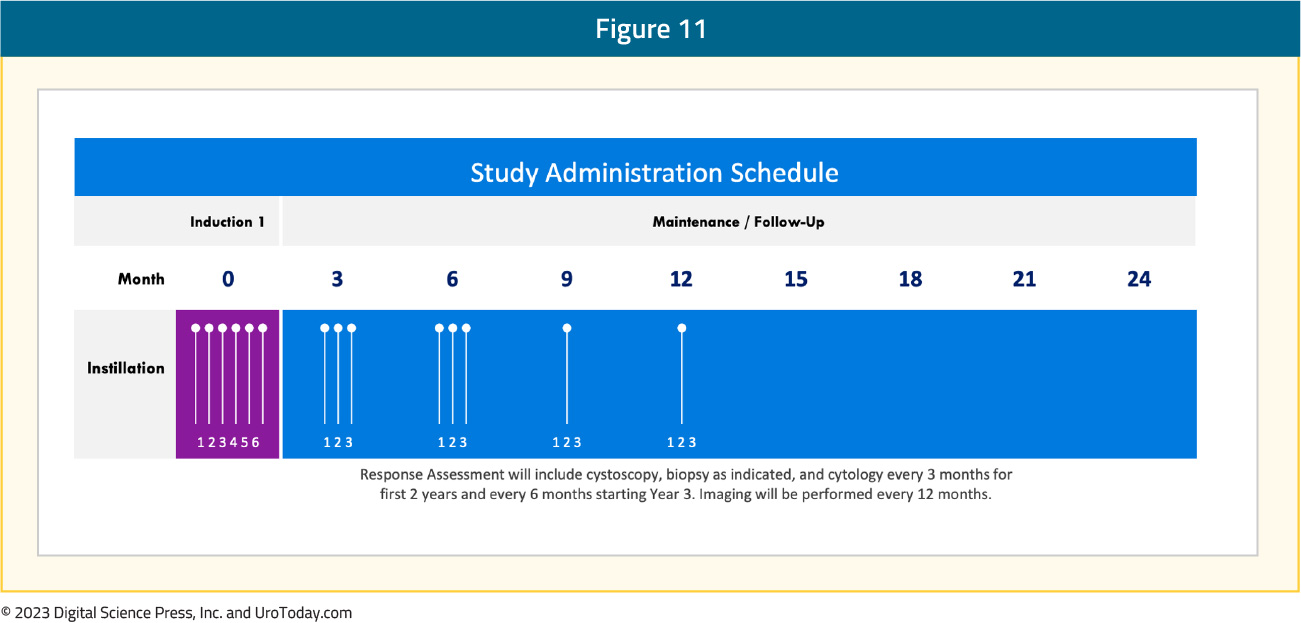
Importantly, this trial will also assess patient reported outcomes and health related quality of life metrics. The study administration schedule includes a weekly 6 week induction phase, 3 weekly maintenance doses after induction, 3 weekly maintenance doses during months 3-6, one maintenance treatment during months 6-9, and one maintenance treatment during months 9-12:
Given the lack of translational data in this disease space, PIVOT-006 also has a robust translational plan, including urine and serum being tested at identified time points: 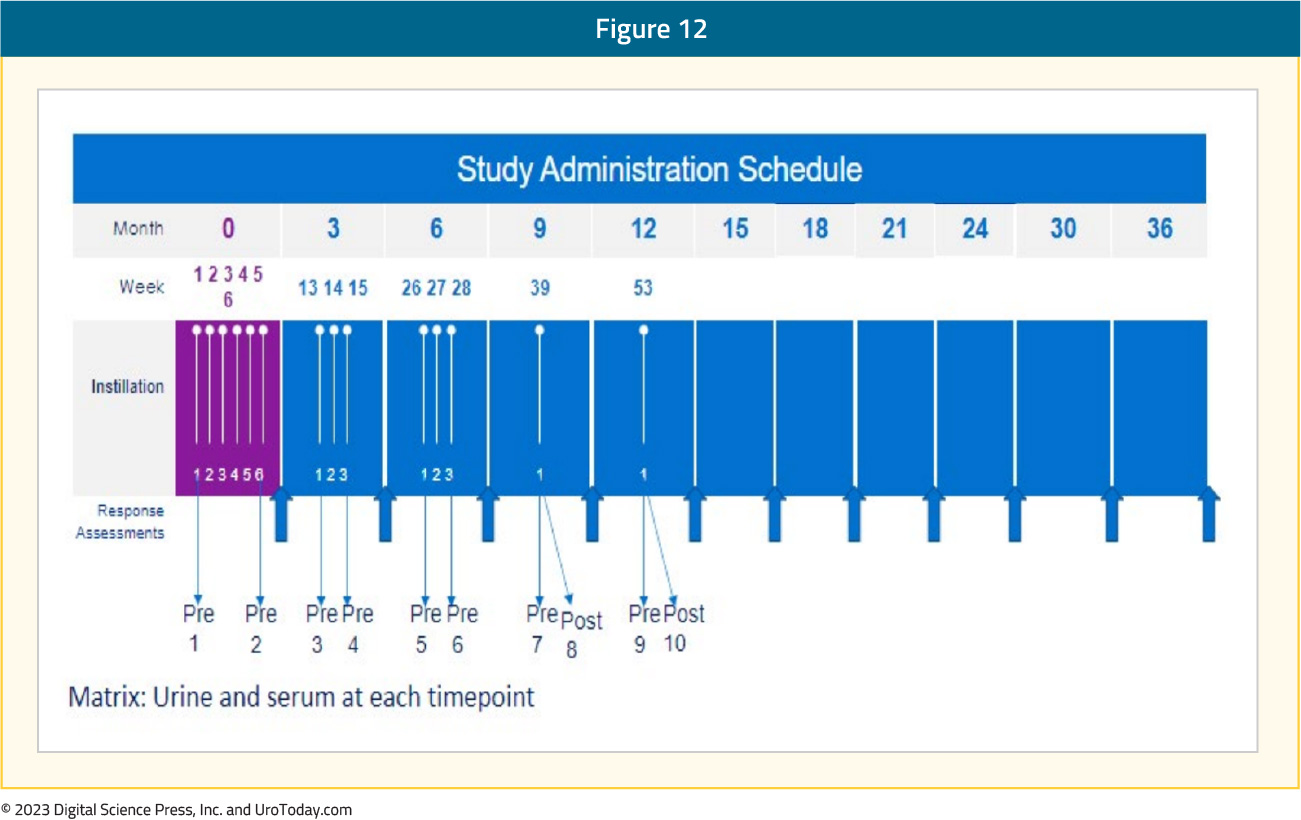
Based on the experience of previous cretostimogene trials, PIVOT-006 trial has streamlined the intravesical installation process. This includes ~100 mL of DDM with a 15 min dwell time followed by ~100 mL of cretostimogene for a 1 hour dwell time. The Foley catheter may be removed if the principal investigator feels the patient will tolerate instillation, and the patient may be observed outside of the procedure room. There has been tremendous support for the PIVOT-006 trial, including support from the SUO-CTC, BCAN, and Parexel Biotech. Currently, there are over 90 North American sites that are registered to be part of the trial: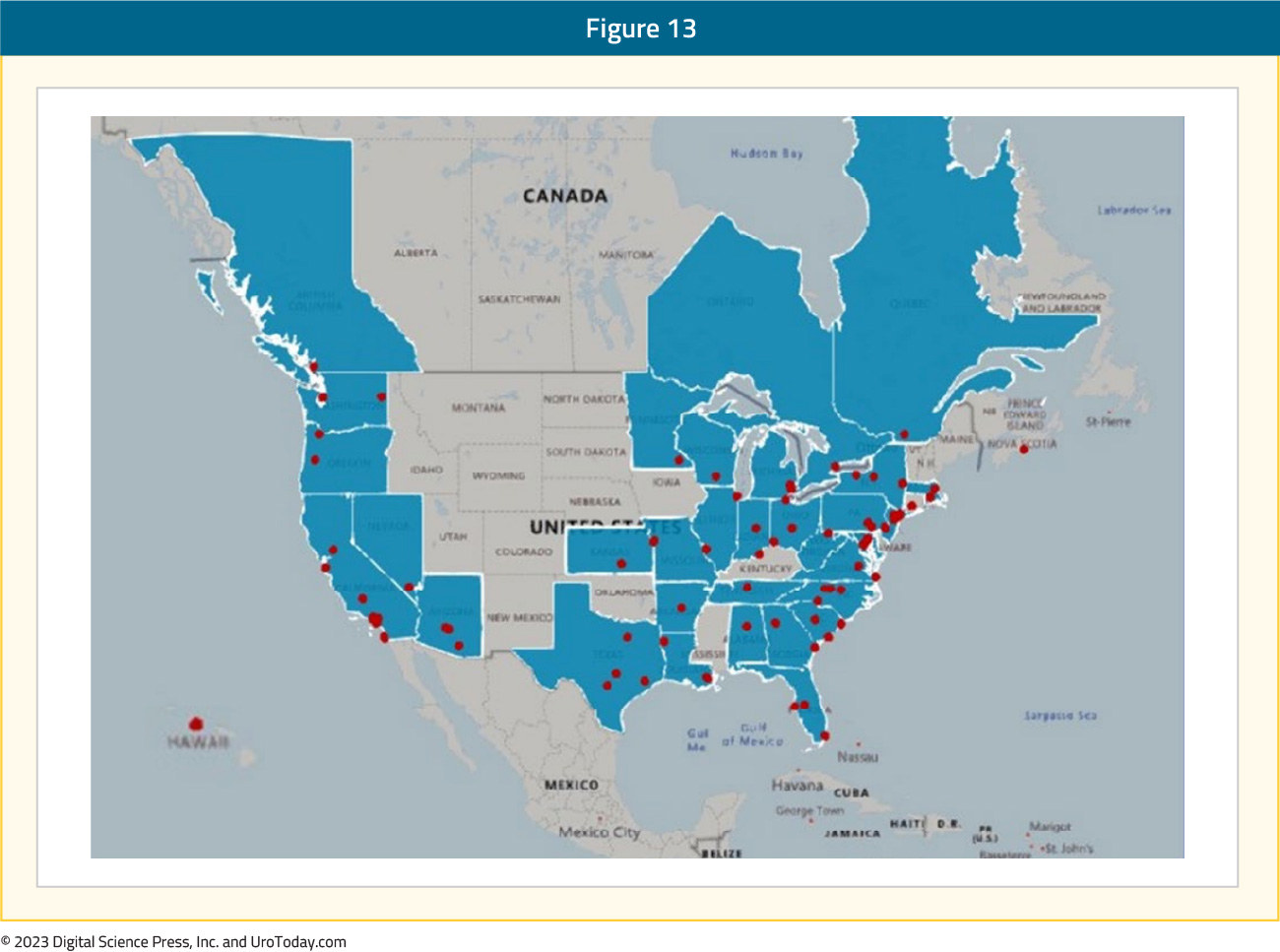
Several factors are keys to success for PIVOT-006:
- Documentation of intermediate risk diagnosis, which relies on provision of timely and complete source data, and appropriate confirmation of intermediate risk NMIBC history
- A streamlined DDM instillation process, which reduces the number of steps, and removal of the Foley catheter after cretostimogene instillation
- Biomarker assessments
- Cytologic assessments/endpoint assessments
Additionally, there are several planned activities to assist with patient enrollment:
- PIVOT-006 will be a featured clinical trial on the BCAN dashboard
- The SUO-CTC will assist with enrollment, with discussions at the SUO annual meeting, as well as emails, social media posts, etc
- Provide each site with resources following IRB review and review by each site:
- Patient postcard
- Doctor discussion guide
- An email for sites to send out
- A PowerPoint presentation on bladder cancer, clinical trials, and PIVOT-006
- Newsletter content
Conclusions
The NMIBC disease space is an exciting space, with many new advances moving forward in BCG-unresponsive NMIBC. However, intermediate risk NMIBC remains an important and treatment orphaned disease space, with very few novel treatment options. PIVOT-006 is designed specifically for potentially adding options to the intermediate risk NMIBC treatment armamentarium. With excellent support from the SUO-CTC and the trial sponsor CG Oncology, there is optimism that this trial will accrue efficiently and we eagerly await the results of this registration trial.
Published December 2023